¶ Irritable Bowel Syndrome (IBS), SIBO, Bloating, and Motility Disorders: Deep Dive
¶ TL;DR
- Verdict: Chronic abdominal pain and altered bowel habits are primary hallmarks of disorders of gut-brain interaction (DGBIs), driven by gut-brain axis dysregulation, visceral hypersensitivity, and impaired gastrointestinal motility.
- Target Population: Clinicians and advanced patients managing chronic bloating, distension, alternating bowel patterns, and suspected small bowel dysbiosis.
- Magnitude & Timeline: Therapeutic response timelines range from 2 to 6 weeks for dietary elimination pathways, while pharmacological or herbal antimicrobial regimens typically achieve SIBO clearance and symptomatic resolution within 10 to 14 days.
- Key Risks: Overtreatment based on false-positive breath tests, mucosal dysbiosis from prolonged restriction diets, and failure to screen for organic "Red Flag" conditions (e.g., celiac disease, inflammatory bowel disease, colorectal malignancy).
- Next Steps: Perform primary differential screening, establish the baseline clinical phenotype using Rome IV criteria, and sequence interventions from dietary modification to prokinetic or antimicrobial therapies.
¶ Quick Answer
Irritable Bowel Syndrome (IBS) and Small Intestinal Bacterial Overgrowth (SIBO) represent overlapping functional and microbiological disorders characterized by visceral hypersensitivity, altered gut motility, and small intestinal fermentation. Diagnostic classification utilizes the Rome IV criteria to segment IBS into four subtypes based on stool consistency. SIBO diagnostics rely on breath-testing gas curves (Hydrogen, Methane, and Hydrogen Sulfide) with a strict 90-minute cutoff to differentiate small intestinal fermentation from normal colonic colocalization. Successful management requires a structured clinical sequence: identifying "Red Flag" symptoms, ruling out structural/inflammatory diseases, implementing targeted dietary pathways (such as the Low-FODMAP diet), resolving dysbiosis via targeted antimicrobial therapies, and maintaining gastrointestinal transit via prokinetic activation of the Migrating Motor Complex (MMC).
¶ What It Is: Pathophysiology & Mechanisms
¶ Rome IV Criteria & IBS Subtypes
Irritable Bowel Syndrome is classified as a Disorder of Gut-Brain Interaction (DGBI) under the Rome IV consensus [1]. The diagnostic criteria require recurrent abdominal pain occurring on average at least 1 day per week in the last 3 months, associated with two or more of the following:
- Relation to defecation (either improvement or worsening).
- Association with a change in frequency of stool.
- Association with a change in form (appearance) of stool.
Symptoms must have started at least 6 months prior to diagnosis. Classification into clinical subtypes depends on the proportion of abnormal bowel movements utilizing the Bristol Stool Form Scale (BSFS) during symptomatic days [2][3]:
- IBS-C (Constipation-predominant): Over 25% of bowel movements are Bristol Stool Scale Type 1 or 2 (hard, lumpy), and less than 25% are Type 6 or 7 (loose, watery).
- IBS-D (Diarrhea-predominant): Over 25% of bowel movements are Bristol Stool Scale Type 6 or 7, and less than 25% are Type 1 or 2.
- IBS-M (Mixed/Alternating): Over 25% of bowel movements are Type 1 or 2, and over 25% are Type 6 or 7.
- IBS-U (Unclassified): Patients meet Rome IV diagnostic criteria for IBS, but bowel habits cannot be accurately categorized into C, D, or M.
¶ Physiological Drivers of IBS
The underlying pathophysiology of IBS is multifactorial and highly individualized:
- Gut-Brain Axis Dysregulation: Bidirectional communication between the central nervous system (CNS) and the enteric nervous system (ENS) is altered. Dysregulation of the hypothalamic-pituitary-adrenal (HPA) axis leads to elevated stress responses, which alter intestinal motility, mucosal immunity, and visceral perception.
- Visceral Hypersensitivity: Patients exhibit a lowered nociceptive threshold in the gut wall. This hyperalgesia is mediated by sensitized peripheral afferents (nociceptors), spinal cord amplification, and altered central processing of sensory inputs. Mast cells adjacent to nerve fibers degranulate and release histamine and tryptase, further excitable to enteric nerves [1:1].
- Vagal Tone and Autonomic Dysfunction: Reduced parasympathetic activity (low vagal tone) is frequently observed in IBS-C, leading to delayed gastric emptying and slow colonic transit. Conversely, sympathetic overactivity or hyper-reactive parasympathetic responses can drive the hypermotility seen in IBS-D.
¶ Rome IV IBS Subtypes and Pathophysiological Drivers
The diagram below maps the brain-gut bidirectional communication and highlights the physiological drivers differentiating each of the Rome IV subtypes.
+----------------------------------+
| GUT-BRAIN AXIS NETWORK |
| Bidirectional Vagus Nerve Path |
+-----------------+----------------+
|
+-----------------------+-----------------------+
| |
v v
+-----------------------+ +-----------------------+
| CENTRAL PROCESSING | | ENTERIC RECEPTORS |
| Visceral Hyperalgesia | | Mast Cell Activation |
| HPA Axis Stress-Drive | | Epithelial Integrity |
+-----------+-----------+ +-----------+-----------+
| |
+-----------------------+-----------------------+
|
v
+-----------------------------------------------------------------------+
| ROME IV SUBTYPE SEGREGATION |
| |
| IBS-C (Constipation) : Slow transit; Low vagal tone; Low secretion |
| IBS-D (Diarrhea) : Fast transit; High vagal tone; Hypersecretion |
| IBS-M (Mixed) : Alternating dysmotility; Variable autonomic |
| IBS-U (Unclassified) : Indeterminate pathophysiology and markers |
+-----------------------------------------------------------------------+
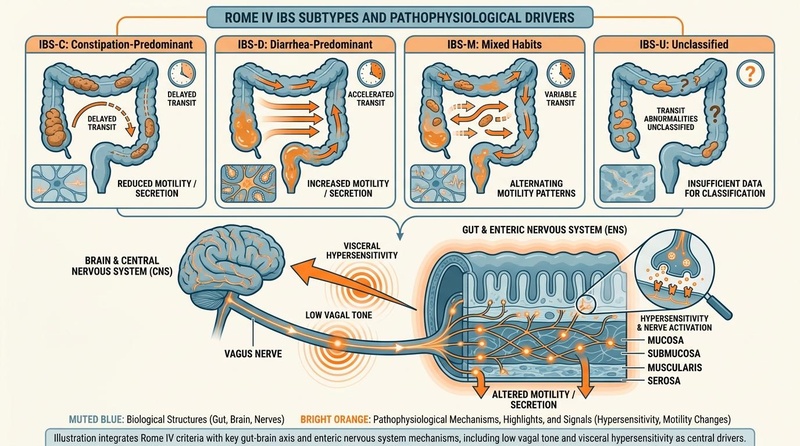
Figure 1: Rome IV IBS Subtypes and Pathophysiological Drivers. Visual plan: Off-white background, muted blue/teal structures representing brain and gut pathways, and subtle bright orange highlights indicating key receptors and visceral pain signaling points.
¶ SIBO Classification & Gas Dynamics
Small Intestinal Bacterial Overgrowth (SIBO) is a clinical form of dysbiosis that occurs when normally low concentrations of bacteria in the small intestine expand, exceeding colony-forming units (CFU)/mL of aspirate, leading to premature fermentation of dietary carbohydrates [4][5]. SIBO is classified into three distinct subtypes based on dominant gas profiles and microbial ecology [4:1]:
- Hydrogen-Dominant SIBO (): Primarily driven by the overgrowth of Gram-negative facultative anaerobes (e.g., Escherichia coli, Klebsiella pneumoniae, Enterobacter spp.) in the small bowel. These bacteria rapidly ferment carbohydrates, releasing large volumes of hydrogen gas [5:1].
- Methane-Dominant SIBO / Intestinal Methanogen Overgrowth (IMO): Driven by archaea, predominantly Methanobrevibacter smithii. Unlike classic bacterial SIBO, IMO can occur in both the small bowel and the colon. Methanogens utilize 4 molecules of hydrogen to produce 1 molecule of methane (). Methane acts as a neuromuscular paralytic in the gut, inhibiting peristalsis and strongly correlating with slow transit and constipation [4:2][6].
- Hydrogen Sulfide SIBO (): Driven by sulfate-reducing bacteria (SRB) such as Desulfovibrio spp. and Bilophila wadsworthia. These microbes compete with methanogens for hydrogen gas to produce toxic hydrogen sulfide (). Excess damages the mitochondrial electron transport chain in colonocytes, degrades the protective mucus barrier, and is strongly associated with diarrhea, visceral pain, and systemic fatigue [7].
¶ Breath Testing Mechanics & Pitfalls
SIBO diagnostics heavily rely on non-invasive breath tests measuring exhaled gases after substrate ingestion (lactulose or glucose) [8].
- The 90-Minute Cutoff Rule: Orally ingested substrate reaches the cecum in approximately 90 minutes in patients with normal oromucosocaecal transit time. Therefore, any rise in Hydrogen () or Hydrogen Sulfide () within 90 minutes indicates fermentation in the small intestine, confirming SIBO [7:1][8:1]. A Methane reading of at any point during the 120-minute test is diagnostic of IMO [4:3][7:2].
- Testing Pitfalls:
- Dietary Prep Bias: Inadequate adherence to a 24-hour low-fermentable diet (restricting fiber, complex carbs, and slow-fermenting sugars) prior to the test can cause elevated baseline gas levels, yielding false-positive results.
- Transit Time Variations: Fast gastric or small bowel transit can deliver the substrate to the colon before 90 minutes, leading to an early colonic rise misdiagnosed as SIBO. Conversely, severe gastroparesis or slow transit can delay delivery, masking a distal small bowel overgrowth.
- Oral Dysbiosis: Microbial fermentation by oral flora can cause a rapid, false gas spike in the first 15–30 minutes of the test.
¶ SIBO Breath Testing Timeline & Substrate Digestion
The chart below illustrates the typical gas concentration curves over a 120-minute testing period, highlighting the critical 90-minute cutoff.
Gas (ppm)
^
| / (Colonic Rise)
50| /
| /
30| * * * / [H2 Positive Threshold: >20 ppm]
| * * /
20|-------------*-----------*----/--------------------------------------
| * * /
10|---------*---------------/-----------------* * * [CH4 Positive: >=10 ppm]
| * / *
+---------------------+---------------------------------------------> Time
0 90 120 min
<--- Small Bowel ----><------ Colonic ----->
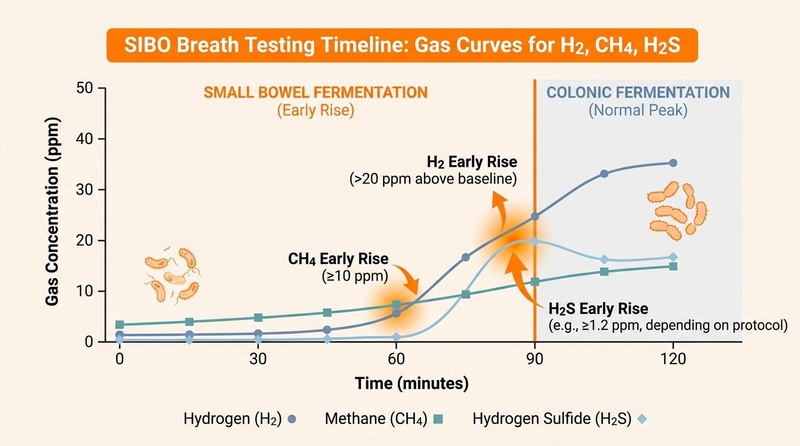
Figure 2: SIBO Breath Testing Timeline & Substrate Digestion. Visual plan: Off-white background, distinct line charts representing Hydrogen (dark blue), Methane (teal), and Hydrogen Sulfide (light blue), with a vertical highlighted orange line at the 90-minute mark to demarcate the small bowel cutoff.
¶ The Migrating Motor Complex (MMC) & Peristalsis
The Migrating Motor Complex (MMC) is a distinct, cyclical pattern of electromechanical activity observed in the gastrointestinal smooth muscle during periods of fasting [9]. The MMC operates under autonomic and enteric nervous system control, repeating every 90 to 120 minutes to sweep residual undigested food, cellular debris, and bacteria down into the colon—acting as the primary physical defense against small intestinal bacterial colonization [9:1].
The MMC cycle consists of four sequential phases [9:2]:
- Phase I (Quiescence): Lasts 45–60 minutes. Characterized by rare action potentials and a near-complete absence of contractions.
- Phase II (Irregular Contractions): Lasts 30–45 minutes. Characterized by random, low-amplitude contractions. Secretions of bile and pancreatic enzymes increase. Activity is modulated by ghrelin and enteric pathways.
- Phase III (The "Housekeeper Wave"): Lasts 5–15 minutes. This is the most critical phase for SIBO prevention. It consists of high-frequency, regular, high-amplitude propulsive contractions originating in the stomach or duodenum and migrating down to the ileocecal valve. Driven by the rhythmic pulsatile release of the hormone motilin and coordinated by the enteric nervous system, it clears the lumen of bacteria and debris [9:3].
- Phase IV (Transition): Lasts 5–10 minutes. A brief transition period where contractions decline, leading back to Phase I.
¶ Peristalsis vs. MMC
Peristalsis is a localized reflex triggered by mechanical distension of the gut wall when food is present, characterized by upstream contraction (circular muscle) and downstream relaxation (longitudinal muscle) to move a bolus forward. In contrast, the MMC is a systemic, fasting-state phenomenon that coordinates long stretches of the stomach and small bowel. Disruption of Phase III of the MMC—often caused by post-infectious autoimmunity (e.g., anti-CdtB and anti-vinculin antibodies damaging interstitial cells of Cajal), chronic stress, or hyperglycemia—results in small bowel stasis, providing an ideal environment for bacterial accumulation and SIBO development [9:4].
¶ The Migrating Motor Complex (MMC) 4-Phase Cycle
The diagram below maps the electromechanical progression of the MMC cycle along with receptor targets for prokinetic therapies.
[ Phase I: Quiescence ] --> 45-60 min (Electrically silent)
|
v
[ Phase II: Irregular Activity ] --> 30-45 min (Random contractions; Ghrelin active)
|
v
[ Phase III: Housekeeper Wave ] --> 5-15 min (Propulsive sweeps; Motilin driven)
|
v
[ Phase IV: Transition ] --> 5-10 min (Contraction decay)
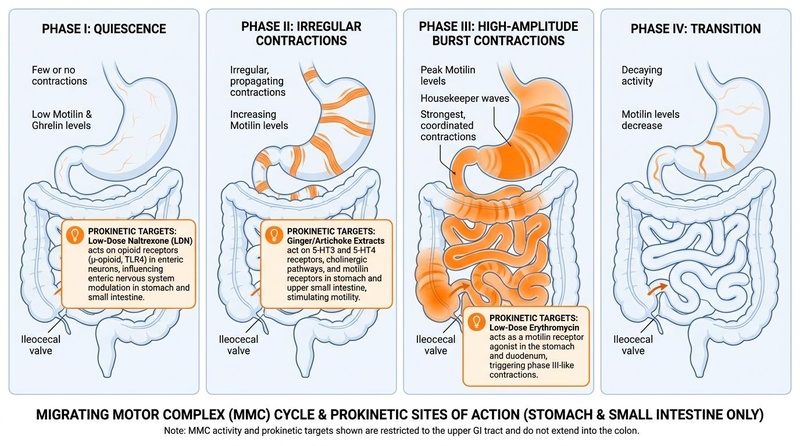
Figure 3: The Migrating Motor Complex (MMC) 4-Phase Cycle and Prokinetic Targets. Visual plan: Off-white background, circular layout showing the 4 phases in muted blue and teal blocks representing the stomach and small intestine, terminating at the ileocecal valve, and bright orange highlights pointing to molecular receptor targets (Motilin, 5-HT4, Ghrelin) where therapeutic agents act. Contractions and prokinetic receptors are strictly located in the upper GI tract and do not extend into the colon.
¶ Does It Work? Evidence Snapshot
¶ Efficacy of GI Interventions
The following table outlines the clinical efficacy, study demographics, and expected effect sizes of major dietary, herbal, and pharmacological interventions used in managing IBS, SIBO, and motility disorders.
| Intervention | Target Outcome | Study Population | Typical Effect Size | Certainty (GRADE) | Key Citations |
|---|---|---|---|---|---|
| Low-FODMAP Diet | Reduction in bloating, pain, diarrhea | IBS-D & IBS-M adults | 50–70% response rate; reduction of IBS Severity Score by points over 4–6 weeks | High | [10][11] |
| Peppermint Oil | Antispasmodic, reduction in pain | Adult IBS (all subtypes) | Relative Risk (RR) of symptom persistent = 0.54 (46% improvement) | Moderate | [12][13] |
| Soluble Fiber (PHGG) | Bowel normalization, flatulence reduction | IBS-C & IBS-D adults | Significant increase in weekly stool frequency; reduction in stool straining | Moderate | [14][15] |
| Rifaximin | Bacterial clearance, bloating reduction | Non-constipated IBS / -SIBO | 41% clinical response rate vs 31% placebo; SIBO eradication rate of 70% | High | [16] |
| Neomycin + Rifaximin | Methane reduction, constipation relief | IMO / Constipation-IBS | 85% methane eradication (to ) and parallel constipation improvement | Moderate | [4:4][16:1] |
| Herbal Antimicrobials (Berberine, Allicin, Oregano) | Bacterial and methanogen eradication | SIBO & IMO adults | Eradication rate equivalent to Rifaximin (~46% on monotherapy) | Low | [17] |
| Prucalopride (High dose: 1-2mg) | Colonic transit acceleration | Chronic Idiopathic Constipation | 3-fold increase in spontaneous complete bowel movements/week | High | [9:5] |
| Low-Dose Naltrexone (LDN, 1-4.5mg) | Pain reduction, motility modulation | Refractory IBS adults | 76% of patients report improvement in pain severity and stool consistency | Low | [18] |
| Ginger + Artichoke Extract | Gastric emptying, MMC stimulation | Functional dyspepsia / SIBO-prone | 24% increase in gastric emptying rate; reduction in postprandial fullness | Moderate | [19][20] |
¶ Who Benefits Most / Least
The clinical manifestations and therapeutic responses in IBS, SIBO, and motility disorders vary significantly across different patient cohorts. Tailoring therapy requires a deep understanding of demographic, hormonal, and physiological variables.
¶ Young Adults (Ages 18–35)
- Most Benefit: This cohort typically shows a high response rate to the Low-FODMAP elimination diet [10:1] and stress-directed enteric therapies (such as gut-directed hypnotherapy or cognitive behavioral therapy) [1:2]. Their baseline symptoms are frequently exacerbated by HPA-axis stress drive, academic or occupational pressure, and irregular circadian/sleep schedules.
- Least Benefit / Risks: Young adults have a higher baseline prevalence of underlying eating disorders or orthorexic tendencies. Restrictive elimination diets must be approached with caution in this group due to the risk of triggering or exacerbating avoidant/restrictive food intake disorder (ARFID).
¶ Men vs. Women
- Hormonal Transits: Progesterone and estrogen receptors are densely expressed throughout the gastrointestinal tract. Elevated progesterone levels (typical of the luteal phase of the menstrual cycle and pregnancy) act as a smooth muscle relaxant, delaying gastric emptying and slowing colonic transit [2:1]. This physiological state exacerbates bloating, gas, and constipation. Conversely, the rapid drop in these hormones pre-menstrually often triggers hypermotility and diarrhea [2:2].
- Subtype Prevalence: Females are disproportionately diagnosed with IBS-C and IMO, which are strongly influenced by hormonal transit delays [1:3][4:5]. Males are more frequently diagnosed with IBS-D, where stress-induced mast cell degranulation and high vagal responses play a dominant role.
- Pregnancy Considerations:
- Low-FODMAP: Safe during pregnancy but must be closely monitored by a clinical dietitian to ensure caloric and micronutrient adequacy.
- Antimicrobials: Rifaximin is poorly absorbed () and is classified as Category C; it should be avoided unless absolutely necessary. Neomycin is contraindicated due to risk of fetal ototoxicity. Standard herbal antimicrobials (such as Berberine and Artemisia) are strictly contraindicated due to potential embryotoxicity and uterine-stimulating properties. soluble fiber (PHGG) and gentle osmotic laxatives are preferred first-line interventions during pregnancy.
¶ Middle-Aged & Older Adults (Ages 50+)
- New-Onset Screening: The presentation of new-onset IBS-like symptoms in patients over the age of 50 is a critical clinical checkpoint. These patients require colonoscopy and imaging to rule out organic pathology (such as colorectal cancer or diverticular disease) before functional IBS can be diagnosed.
- Pelvic Floor Dysfunction: Older adults presenting with chronic constipation often suffer from pelvic floor dyssynergia (paradoxical contraction or failure to relax pelvic floor muscles during defecation) rather than simple slow-transit IBS-C. Laxative or fiber therapies frequently fail in this cohort, whereas anorectal biofeedback therapy yields high clinical efficacy.
- Medication-Induced Transit Delays: Polypharmacy is highly prevalent in older adults. Chronic use of calcium channel blockers (for hypertension), anticholinergics, and opioid analgesics alters gut motility, frequently causing secondary constipation and small bowel stasis that predisposes the patient to SIBO.
¶ How to Try It: Actionable Protocols
Managing IBS and SIBO requires sequential clinical pathways to prevent nutrient deficiencies, avoid chronic dysbiosis, and target the root physiological drivers.
¶ Dietary Pathway: Low-FODMAP Care Pathway
FODMAPs (Fermentable Oligosaccharides, Disaccharides, Monosaccharides, and Polyols) are short-chain carbohydrates that are poorly absorbed in the small intestine, drawing water into the lumen via osmosis and undergoing rapid fermentation by colonic bacteria to produce carbon dioxide, hydrogen, and methane [10:2].
The Low-FODMAP protocol must be executed in three distinct, structured phases to preserve long-term gut health:
+-----------------------------------------------------------+
| DIETARY ASSESSMENT & PREPARATION |
| Rule out eating disorders; establish symptom log |
+-----------------------------+-----------------------------+
|
v
+-----------------------------------------------------------+
| PHASE 1: STRICT ELIMINATION |
| Duration: 2 to 6 weeks |
| Action : Remove all high-FODMAP foods |
| Goal : Achieve >=50% reduction in GI symptoms |
+-----------------------------+-----------------------------+
|
v
+-----------------------------------------------------------+
| PHASE 2: SYSTEMATIC REINTRODUCTION |
| Duration: 6 to 8 weeks |
| Action : Test individual FODMAP groups over 3-day blocks |
| Goal : Identify specific carbohydrate triggers |
+-----------------------------+-----------------------------+
|
v
+-----------------------------------------------------------+
| PHASE 3: SUSTAINABLE PERSONALIZATION |
| Duration: Long-term / Indefinite |
| Action : Reintegrate tolerated FODMAPs to expand diet |
| Goal : Maximize prebiotic intake & microbiome diversity|
+-----------------------------------------------------------+
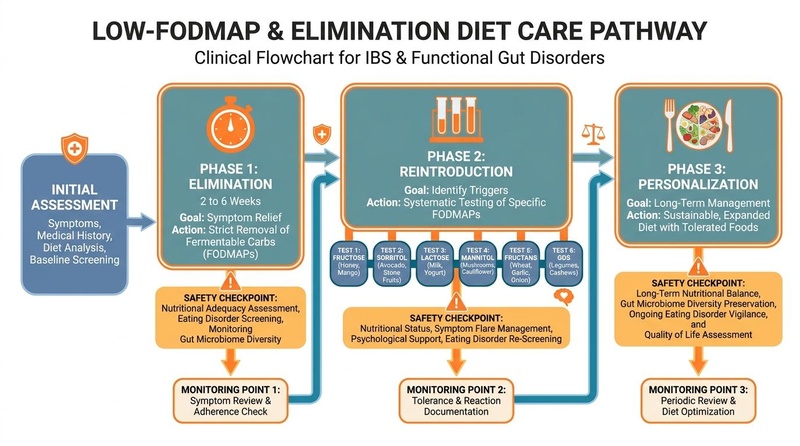
Figure 4: Low-FODMAP & Elimination Diet Care Pathway. Visual plan: Flowchart depicting the assessment and three progressive phases in muted blue/teal blocks, highlighted orange warning icons at critical safety checkpoints (such as symptom & tolerance monitoring, nutritional compliance, and eating disorder screens), and bottom-aligned green monitoring points.
- Phase 1: Strict Elimination (2 to 6 Weeks):
- Action: Remove all high-FODMAP foods. Restrict intake of fructans (wheat, garlic, onions), GOS (legumes), lactose (dairy), fructose (apples, honey), and polyols (sorbitol/mannitol in stone fruits and cauliflowers) [10:3][21].
- Clinical Boundary: This phase is not a long-term diet. Prolonged strict elimination significantly reduces the abundance of beneficial butyrate-producing Bifidobacteria and Faecalibacterium prausnitzii, degrading the mucosal barrier [22]. If symptoms do not improve after 4 weeks of strict adherence, the diet should be discontinued and alternative drivers explored.
- Phase 2: Systematic Reintroduction (6 to 8 Weeks):
- Action: Reintroduce one FODMAP group at a time over a 3-day testing window while maintaining a low-FODMAP baseline.
- Example: Day 1: 1/4 clove garlic (Fructan test); Day 2: 1/2 clove garlic; Day 3: 1 whole clove garlic. Record symptoms. Washout for 3 days before testing the next carbohydrate category (e.g., Lactose, Sorbitol).
- Phase 3: Sustainable Personalization (Long-Term):
- Action: Reintegrate tolerated or moderately tolerated FODMAPs back into the diet to maximize prebiotic variety, maintain gut microbial diversity, and restore quality of life [11:1].
¶ SIBO Eradication Protocols
Selecting the appropriate eradication regimen depends on the patient's breath test gas profile. While standard clinical approaches rely on conventional antibiotics or botanical extracts, research continues to explore endogenous host-defense peptides like LL-37 for their targeted antimicrobial and mucosal immunomodulatory actions in intestinal dysbiosis.
¶ Protocol A: Hydrogen-Dominant SIBO Regimen
- Pharmacological First-Line:
- Rifaximin: 550 mg orally, three times daily (TID) for 14 days [16:2].
- Mechanism: Rifaximin is a non-systemic, bile-soluble antibiotic that concentrates highly in the small bowel. It exhibits minimal systemic absorption (), sparing the colonic microbiome.
- Herbal Alternative (Equivalent efficacy demonstrated in clinical trials [17:1]):
- Berberine Complex: Concentrated berberine extract (e.g., from Berberis aristata or Goldenseal) dosed at 500 mg orally, three times daily (TID) for 30 days [17:2].
- Neem Extract: 300–500 mg orally, three times daily (TID) for 30 days [17:3].
- Oregano Oil (Emulsified): 50–100 mg orally, TID for 30 days.
¶ Protocol B: Methane-Dominant SIBO / IMO Regimen
- Pharmacological First-Line:
- Rifaximin (550 mg TID) + Neomycin (500 mg BID) for 14 days [4:6][16:3].
- Alternative: Rifaximin (550 mg TID) + Metronidazole (250 mg TID) for 14 days [4:7].
- Rationale: Methanogens are archaea and are highly resistant to many standard antibiotics. Adding Neomycin or Metronidazole is required to effectively target and clear methanogenic organisms, restoring transit time.
- Herbal Alternative:
- Allicin (Concentrated extract from garlic): 450 mg orally, three times daily (TID) for 30 days.
- Rationale: Allicin acts as an inhibitor of the archaeal methanogenesis pathway without introducing the high-FODMAP fructans found in raw garlic.
- Combine with a broad-spectrum antimicrobial such as Berberine Complex (500 mg TID) or Neem Extract (500 mg TID) for 30 days [17:4].
¶ Protocol C: Hydrogen Sulfide SIBO Regimen
- Pharmacological First-Line:
- Rifaximin: 550 mg TID for 14 days, combined with Bismuth Subsalicylate (e.g., Pepto-Bismol) dosed at 524 mg, four times daily for 14 days [7:3].
- Rationale: Bismuth acts as a direct sulfide scavenger, binding to volatile hydrogen sulfide in the intestinal lumen to neutralize its toxicity to the mucosal lining.
- Herbal Alternative:
- Oregano Oil (Emulsified) + Uva Ursi: Dosed concurrently for 30 days alongside heavy supplementation of Bismuth (e.g., Bismuth citrate, 150–300 mg TID).
¶ Biofilm Disruption (Optional Adjuvant)
- In chronic or highly refractory cases of SIBO/IMO, bacteria can organize into protective extracellular polymeric substance (EPS) matrices (biofilms), reducing antibiotic penetration [23].
- Protocol: Administer a biofilm-disrupting agent containing bismuth subsalicylate, thiol donors, or enzymes (e.g., bismuth-thiol complexes, alpha-galactosidase, cellulase) 30 minutes before antimicrobial dosing to expose bacterial populations [23:1].
¶ Prokinetic & MMC Maintenance Protocols
Preventing SIBO recurrence requires active restoration of gastric and small intestinal motility immediately following antimicrobial eradication therapy. Prokinetics should be administered at night before bed (after a minimum 3-4 hour fast) to maximize the overnight Migrating Motor Complex [9:6].
- Option A: Pharmacological 5-HT4 Agonist:
- Prucalopride (low dose): 0.5 mg to 1.0 mg orally once daily, administered at bedtime [9:7].
- Mechanism: Prucalopride is a highly selective serotonin 5-HT4 receptor agonist. At low doses, it selectively stimulates enteric cholinergic neurons to trigger Phase III of the MMC without the cardiovascular risks associated with older non-selective agonists.
- Option B: Low-Dose Naltrexone (LDN):
- Naltrexone: 1.5 mg to 4.5 mg orally once daily, administered at bedtime [18:1].
- Mechanism: Blockade of opioid receptors by low-dose naltrexone triggers a transient increase in endogenous met-enkephalin release and upregulates receptor density. This pathway modulates gut inflammation, reduces visceral hypersensitivity, and coordinates smooth muscle contractions.
- Option C: Low-Dose Motilin Agonist:
- Erythromycin (low dose): 50 mg to 100 mg orally once daily at bedtime [9:8].
- Mechanism: At sub-antimicrobial doses, erythromycin binds directly to motilin receptors on enteric smooth muscle, mimicking endogenous motilin to trigger a powerful Phase III housekeeper wave.
- Option D: Standard Botanical Prokinetic:
- Ginger + Artichoke Leaf Extract: A combination extract containing 20–30% gingerols and cynarin (e.g., Prodigest) dosed at 100–200 mg, taken twice daily: once before the largest meal of the day and once at bedtime [19:1][20:1].
- Mechanism: Ginger stimulates cholinergic pathways and acts as a natural 5-HT3 receptor antagonist (accelerating gastric emptying), while artichoke cynarin promotes bile flow and acts as a mild duodenal prokinetic [19:2].
¶ Safety, Interactions, Red Flags
¶ Primary Diagnostic Safety
Functional gut protocols must only be implemented after structural and inflammatory organic pathologies have been excluded through appropriate medical diagnostic pathways.
- Primary Differential Screening: Before establishing a diagnosis of IBS, clinical guidelines recommend screening for:
- Celiac Disease: Via IgA tissue transglutaminase (tTG) and total serum IgA (while on a gluten-containing diet).
- Inflammatory Bowel Disease (IBD): Via fecal calprotectin (elevations warrant endoscopic evaluation) and C-reactive protein (CRP).
- Colorectal Malignancy: Via age-appropriate colonoscopy screening.
¶ Clinical "Red Flags"
The presence of any of the following "Red Flag" symptoms indicates potential structural, inflammatory, or neoplastic pathology. These findings necessitate immediate referral for diagnostic workup and exclude primary self-directed functional protocols:
- Onset of symptoms after age 50 in a previously asymptomatic patient.
- Unexplained, progressive weight loss ( of body weight within 6 months).
- Nocturnal diarrhea (waking from sleep to defecate, suggesting secretory organic pathology).
- Hematochezia (rectal bleeding/blood in stool) or melena (black, tarry stools).
- Unexplained iron-deficiency anemia.
- Unexplained persistent fever or systemic inflammatory signs.
- Family history of colorectal cancer, inflammatory bowel disease, or celiac disease.
- Palpable abdominal or rectal mass on physical examination.
¶ Treatment-Specific Safety Profiles & Adverse Events
- Low-FODMAP Diet Risks:
- Adverse Events: Nutrient deficiency (calcium, folate, B vitamins), severe dysbiosis (depletion of prebiotic-dependent Bifidobacterium species) [22:1], and psychosocial isolation.
- Absolute Contraindications: History of eating disorders (Anorexia Nervosa, Bulimia Nervosa, ARFID).
- Rifaximin Profile:
- Adverse Events: Mild headache, flatulence, nausea, abdominal pain.
- Safety: Extremely high safety profile with low risk of systemic resistance due to lack of absorption and concentration in bile.
- Neomycin Profile:
- Adverse Events: Ototoxicity (vestibular and cochlear damage), nephrotoxicity, neuromuscular blockade.
- Safety: Neomycin has very low systemic absorption but should be avoided in patients with renal impairment, pre-existing hearing loss, or those taking other ototoxic medications (such as aminoglycosides or loop diuretics).
- Herbal Antimicrobials (Berberine, Allicin, Oregano) Risks:
- Berberine: Potent inhibitor of CYP2D6, CYP3A4, and CYP2C9 enzymes. It must not be administered concurrently with medications cleared by these pathways (e.g., cyclosporine, warfarin, certain beta-blockers). Berberine is a smooth muscle stimulant and is strictly contraindicated during pregnancy due to the risk of inducing uterine contractions.
- Emulsified Oregano Oil: Highly mucosal-irritating if taken long-term; can lead to localized mucosal inflammation. Should not be used continuously for more than 4 to 6 weeks.
- Prokinetics Safety:
- Prucalopride: Common side effects include transient headache (typically resolves within 48 hours), nausea, abdominal cramps, and diarrhea. Avoid in patients with severe inflammatory bowel conditions, intestinal perforation, or obstructive mechanical disorders.
- Low-Dose Erythromycin: Can prolong the QTc interval at high doses, though rare at sub-antimicrobial doses (50–100 mg). Use caution if co-administering with strong CYP3A4 inhibitors (which increase erythromycin concentrations).
¶ Tracking & What "Good" Looks Like
Symptom relief and clinical success in IBS and SIBO management are tracked via a combination of objective biomarker markers, stool metrics, and highly structured N-of-1 self-experimentation templates.
¶ Objective & Subjective Biomarkers
- Breath Test Re-Testing (Objective): A post-treatment breath test should be performed if symptoms persist. Successful eradication is defined as a reduction of Hydrogen gas to and Methane gas to within the 90-minute testing window [4:8][8:2].
- Fecal Calprotectin: Used to confirm that symptomatic improvements correlate with a lack of intestinal inflammation (calprotectin should remain ).
- Bristol Stool Form Scale (Subjective): Track daily bowel habits. The clinical goal is to normalize stool consistency to Bristol Types 3 or 4, with a dramatic reduction in Type 1-2 (constipation) and Type 6-7 (diarrhea).
- Subjective Severity Scales: Utilizing tools like the IBS Symptom Severity Score (IBS-SSS) to track:
- Abdominal pain intensity (0–100 scale).
- Abdominal pain frequency (number of days in a 10-day period).
- Severity of abdominal distension/bloating.
- Dissatisfaction with bowel habits.
- Impact of bowel habits on general life.
¶ Clinical Timeline Expectations
- Time-to-Benefit:
- Dietary Pathway: Bloating and pain reduction typically occur within 7 to 14 days of Phase 1 Low-FODMAP initiation [10:4].
- SIBO Antimicrobial Therapies: Symptom improvement is typically seen on Days 5 to 10 of a 14-day cycle. A "die-off" reaction (Herxheimer-like response, characterized by transiently worsening bloating, fatigue, and headache) can occur during the first 3–5 days due to bacterial lysis and lipopolysaccharide release.
- Prokinetics: Improvement in bowel frequency and reduction in morning bloating are expected within 1 to 2 weeks of starting a bedtime prokinetic [9:9].
- Time-to-Washout:
- Low-FODMAP: Reintroduction of fermentable carbohydrates typically triggers symptoms within 12 to 24 hours if the carbohydrate is a true physiological trigger.
- Prucalopride: Colonic transit times return to baseline within 48 to 72 hours of drug discontinuation.
¶ N-of-1 Personalization Template
To systematically identify specific dietary or prokinetic triggers, clinicians utilize an A/B/A withdrawal template.
+-----------------------------------------------------------------------------+
| N-of-1 TEMPLATE |
+----------------------+------------------------------+-----------------------+
| WEEK 1 (Baseline) | WEEK 2-3 (Active) | WEEK 4 (Withdrawal) |
| | | |
| - High-FODMAP diet | - Implement intervention | - Remove active |
| - No prokinetics | (e.g. Low-FODMAP, LDN, | intervention |
| - Log daily: | or Ginger/Artichoke) | - Revert to baseline |
| * BSFS Type | - Log daily: | - Log daily: |
| * Pain (0-10) | * BSFS Type | * BSFS Type |
| * Bloating (0-10) | * Pain (0-10) | * Pain (0-10) |
| | * Bloating (0-10) | * Bloating (0-10) |
+----------------------+------------------------------+-----------------------+
- Inclusion Rule: If symptoms resolve during Week 2–3, revert to baseline during Week 4, and return to baseline severity within 4 days, the intervention is deemed a true clinical responder.
¶ Common Mistakes & Myths
- Mistake 1: Staying on the Strict Low-FODMAP Diet Indefinitely
- Reality: Many patients achieve excellent symptom relief during Phase 1 (Elimination) and choose to remain on the strict diet indefinitely out of fear of symptom recurrence. This is a critical clinical error. Prolonged restriction deprives the colonic microbiome of essential prebiotic fibers, leading to a severe decline in short-chain fatty acid (SCFA) production, degradation of the mucosal barrier, and systemic dysbiosis [22:2]. Phase 2 (Reintroduction) must be initiated by Week 6.
- Mistake 2: Failing to Use a Prokinetic Post-SIBO Eradication
- Reality: SIBO is not a primary disease; it is a symptom of an underlying failure of the gut's clearance mechanisms—most commonly a damaged Migrating Motor Complex (MMC) [9:10]. Treating SIBO with antibiotics alone without implementing a post-eradication prokinetic leads to a recurrence rate of up to 60% within 3 months, as residual bacteria rapidly recolonize the stagnant small bowel.
- Mistake 3: Relying on Probiotics During an Active SIBO Flare
- Reality: Ingesting billions of CFU of standard probiotics (especially those containing lactic-acid producing Lactobacillus or Bifidobacterium strains) while the small intestine is actively overgrown can worsen symptoms. Introducing more bacteria into a stagnant, fermenting small bowel often increases gas production, bloating, and D-lactate levels. Probiotics should be reserved for the post-eradication phase to help restore colonic diversity.
- Myth 4: "All Bloating is SIBO"
- Reality: While SIBO is a common cause of chronic bloating, several other factors can drive this symptom, including visceral hypersensitivity, abdominal phrenic dyssynergia (abnormal diaphragmatic contraction and abdominal wall relaxation during gas production), delayed gastric emptying, pelvic floor dysfunction, and food intolerances. A positive breath test is required to confirm SIBO before initiating antimicrobial therapies.
¶ Decision Tree
Is the patient presenting with chronic bloating,
distension, abdominal pain, or bowel changes?
|
v
+-----------------------------------------------+
| Are any Clinical Red Flags present? |
| (Age >50, weight loss, blood, anemia, fever) |
+-----------------------+-----------------------+
|
+------------------------+------------------------+
| Yes | No
v v
+----------------------------+ +----------------------------+
| Halt protocol immediately. | | Screen for differentials: |
| Refer for conventional | | Celiac (tTG), IBD (Fecal |
| gastroenterology diagnostic | | Calprotectin), Thyroid. |
| workup. | +--------------+-------------+
+----------------------------+ |
+-------------------------+
v
Are inflammatory markers elevated?
|
+------------------------+------------------------+
| Yes | No
v v
+----------------------------+ +----------------------------+
| Refer for specialist IBD | | Diagnose IBS per Rome IV |
| evaluation. | | and perform 3-Gas Breath |
+----------------------------+ | Test (H2, CH4, H2S). |
+--------------+-------------+
|
+------------------------------+------------------------------+
v v v
Hydrogen Positive (>20ppm) Methane Positive (>=10ppm) H2S Positive (>=1.2ppm)
| | |
v v v
[Hydrogen SIBO] [IMO] [H2S SIBO]
| | |
+------------------------------+------------------------------+
|
v
+----------------------------+
| 1. Initiate 14-day targeted|
| antimicrobial regimen. |
| 2. Implement Low-FODMAP |
| diet for symptom relief.|
| 3. Follow immediately with |
| bedtime prokinetics and |
| biofilm disruption if |
| indicated. |
+----------------------------+
¶ FAQs
- Q: Can I use Saccharomyces boulardii during SIBO treatment?
- A: Yes. Unlike bacterial probiotics, Saccharomyces boulardii is a non-pathogenic, transient biotherapeutic yeast that is highly resistant to both pharmacological and herbal antimicrobials. Clinical evidence indicates that co-administration of S. boulardii with rifaximin significantly reduces antibiotic-associated diarrhea, helps degrade bacterial toxins, and limits fungal overgrowth (Candida) during therapy [6:1].
- Q: How long does a "die-off" reaction last, and how can I manage it?
- A: A die-off (Herxheimer) reaction typically lasts 3 to 5 days. It occurs as large numbers of bacteria are killed, releasing immunogenic lipopolysaccharides (LPS) that trigger transient systemic inflammation. Symptoms can be managed by ensuring adequate hydration, supplementing with activated charcoal or binders (taken 2 hours away from medications/meals), and temporary reduction of antimicrobial dosages.
- Q: Will a prokinetic make my diarrhea-predominant IBS (IBS-D) worse?
- A: It depends on the agent. While strong colonic prokinetics (like high-dose prucalopride) will accelerate transit and worsen diarrhea, low-dose naltrexone (LDN) is often well-tolerated in IBS-D. LDN modulates visceral hypersensitivity and gut inflammation without causing hypermotility [18:2]. Additionally, botanical prokinetics like ginger act primarily on the stomach and proximal duodenum, stimulating the fasting MMC without accelerating distal colonic transit.
- Q: What is the difference between a glucose and a lactulose breath test?
- A: Glucose is rapidly absorbed in the proximal small bowel. Therefore, a glucose breath test is highly specific for proximal SIBO but can miss bacterial overgrowth in the distal ileum [8:3]. Lactulose cannot be absorbed by humans and travels the entire length of the gastrointestinal tract, making it highly sensitive for detecting distal small bowel overgrowth, though it carries a slightly higher risk of false-positives if the patient has rapid intestinal transit [8:4].
- Q: Can chronic stress cause SIBO?
- A: Yes. Under chronic stress, the hypothalamic-pituitary-adrenal (HPA) axis activates the sympathetic nervous system, shifting blood flow away from the gut and inhibiting parasympathetic vagal tone [1:4]. This directly suppresses the release of motilin and shuts down Phase III of the Migrating Motor Complex (MMC), leading to small intestinal stasis and allowing colonic bacteria to migrate upward and colonize the small bowel.
¶ Glossary
- Disorder of Gut-Brain Interaction (DGBI): A class of gastrointestinal disorders characterized by structural normalcy but functional dysregulation of gut-brain axis communication, visceral sensation, and motility.
- Migrating Motor Complex (MMC): A cyclical, electromechanical pattern of contractions occurring in the stomach and small intestine during fasting that clears residual food and prevents bacterial colonization.
- Visceral Hypersensitivity: A lowered threshold for pain and discomfort in the internal organs, leading to a hyper-reactive nociceptive response to normal gastrointestinal processes.
- FODMAPs: Fermentable Oligosaccharides, Disaccharides, Monosaccharides, and Polyols. Short-chain carbohydrates that are poorly absorbed and rapidly fermented in the gastrointestinal tract.
- Intestinal Methanogen Overgrowth (IMO): Overgrowth of methane-producing archaea (Methanobrevibacter smithii) in the small and/or large bowel, strongly associated with chronic constipation.
- Motilin: A peptide hormone secreted by duodenal endocrine M cells that triggers the cyclic Phase III "housekeeper waves" of the Migrating Motor Complex.
- Bristol Stool Form Scale (BSFS): A diagnostic tool designed to classify human feces into seven distinct categories, serving as a reliable surrogate marker for gastrointestinal transit time.
¶ Methods: Search Strategy & Evidence-Grading Rubric
¶ Search Strategy
- Databases: PubMed, MEDLINE, Cochrane Database of Systematic Reviews, ClinicalTrials.gov.
- Search Windows: Database inception through June 2026.
- Search Strings:
"irritable bowel syndrome" AND "Rome IV criteria" AND "subtypes""small intestinal bacterial overgrowth" AND "breath testing" AND ("methane" OR "hydrogen" OR "hydrogen sulfide")"migrating motor complex" AND "prokinetics" AND ("erythromycin" OR "prucalopride" OR "naltrexone")"low FODMAP diet" AND "irritable bowel syndrome" AND "systematic review""SIBO" AND "herbal antimicrobials" AND "rifaximin" AND "neomycin"
- Inclusion Rules: Meta-analyses, randomized controlled trials (RCTs), prospective cohort studies, and consensus guidelines. Animal model studies and in vitro papers were excluded from the primary outcomes matrix.
¶ Evidence-Grading Rubric
The certainty of evidence for each therapeutic intervention was assessed utilizing the GRADE (Grading of Recommendations Assessment, Development and Evaluation) framework:
- High Certainty: Multiple large, high-quality RCTs with consistent results or well-conducted systematic reviews. Further research is very unlikely to change our confidence in the estimate of effect.
- Moderate Certainty: 1 or 2 medium-sized RCTs with minor limitations, or large, high-quality prospective observational studies. Further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate.
- Low Certainty: Small, uncontrolled clinical trials, retrospective studies, or pilot studies with significant design limitations. Any estimate of effect is highly uncertain.
¶ References
¶ Update Log
¶ July 6, 2026
- Diagnostic & Therapeutic Deep Dive: Established comprehensive baseline analysis utilizing Rome IV criteria [2:3].
- Gas Curve Visualizations: Integrated 3-gas breath-testing timeline mechanics with the 90-minute cutoff [16:4].
- MMC Motility Integration: Outlined the 4-phase Migrating Motor Complex cycle and receptor-level targets for prucalopride and erythromycin [9:11].
- Evidence Snapshot Matrix: Created structured outcome table mapping GRADE certainties and effect sizes across standard clinical and botanical pathways [10:5][12:1][17:5][19:3].
Törnblom H, Drossman DA. Psychopharmacologic Therapies for Irritable Bowel Syndrome. Gastroenterology Clinics of North America. 2021. https://pubmed.ncbi.nlm.nih.gov/34304793/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Luo J, To WLW, Xu Q. Clinical practice guidelines for the diagnosis of constipation-predominant irritable bowel syndrome and functional constipation in adults: a scoping review. BMC Gastroenterology. 2025. https://pubmed.ncbi.nlm.nih.gov/40205539/ ↩︎ ↩︎ ↩︎ ↩︎
Cymbal M, Chatterjee A, Ajayi-Fox P. Specialty laboratory testing for chronic abdominal pain in irritable bowel syndrome. Scandinavian Journal of Gastroenterology. 2025. https://pubmed.ncbi.nlm.nih.gov/39853154/ ↩︎
Iftequar Y, Bajpai P, Dav R. Targeted antibiotic and dietary approaches in managing small intestinal bacterial overgrowth across irritable bowel syndrome subtypes. Internal and Emergency Medicine. 2026. https://pubmed.ncbi.nlm.nih.gov/42310284/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Wang Z, Tan W, Zhang P. Potential subtype-specific alterations in gut microbiota and branched-chain amino acid metabolism in hydrogen- and methane-predominant small intestinal bacterial overgrowth. Scientific Reports. 2026. https://pubmed.ncbi.nlm.nih.gov/41857155/ ↩︎ ↩︎
Maev IV, Andreev DN, Shaburov RI. Study on the efficacy of combination therapy with rifaximin and Saccharomyces boulardii CNCM I-745 in patients with small intestinal bacterial overgrowth associated with long-term use of proton pump inhibitors. Terapevticheskii Arkhiv. 2025. https://pubmed.ncbi.nlm.nih.gov/40884341/ ↩︎ ↩︎
Ruscio M, Guard G, O'Dwyer D. Biofilm Disruption Enhances Antimicrobial Therapy for Small Intestinal Bacterial Overgrowth and Intestinal Methanogen Overgrowth. Cureus. 2025. https://pubmed.ncbi.nlm.nih.gov/41394228/ ↩︎ ↩︎ ↩︎ ↩︎
Scalese G, Spina L, Gallucci L. Diagnostic Evaluation of Small Intestinal Microbial Overgrowth: A Cross-Sectional Comparison of Glucose and Lactulose Breath Tests. Journal of Clinical Medicine. 2025. https://pubmed.ncbi.nlm.nih.gov/41464822/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Mustafa F, Noor R, Murtaza A. Small Intestinal Bacterial Overgrowth (SIBO) - Prevention and Therapeutic Role of Nutrition, Prebiotics, Probiotics, and Prokinetics. Current Pharmaceutical Design. 2025. https://pubmed.ncbi.nlm.nih.gov/40296627/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Jent S, Bez NS, Haddad J. The efficacy and real-world effectiveness of a diet low in fermentable oligo-, di-, monosaccharides and polyols in irritable bowel syndrome: A systematic review and meta-analysis. Clinical Nutrition. 2024. https://pubmed.ncbi.nlm.nih.gov/38754307/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Pouladi A, Arabpour E, Bahrami O. Impacts of the Long-Term Low-FODMAP Diet in Patients With Irritable Bowel Syndrome: A Systematic Review and Meta-Analysis. Journal of Human Nutrition and Dietetics. 2025. https://pubmed.ncbi.nlm.nih.gov/40735813/ ↩︎ ↩︎
Ingrosso MR, Ianiro G, Nee J. Systematic review and meta-analysis: efficacy of peppermint oil in irritable bowel syndrome. Alimentary Pharmacology & Therapeutics. 2022. https://pubmed.ncbi.nlm.nih.gov/35942669/ ↩︎ ↩︎
Alammar N, Wang L, Saberi B. The impact of peppermint oil on the irritable bowel syndrome: a meta-analysis of the pooled clinical data. BMC Complementary and Alternative Medicine. 2019. https://pubmed.ncbi.nlm.nih.gov/30654773/ ↩︎
Giannini EG, Mansi C, Dulbecco P. Role of partially hydrolyzed guar gum in the treatment of irritable bowel syndrome. Nutrition. 2006. https://pubmed.ncbi.nlm.nih.gov/16413751/ ↩︎
Yasukawa Z, Inoue R, Ozeki M. Effect of Repeated Consumption of Partially Hydrolyzed Guar Gum on Fecal Characteristics and Gut Microbiota: A Randomized, Double-Blind, Placebo-Controlled, and Parallel-Group Clinical Trial. Nutrients. 2019. https://pubmed.ncbi.nlm.nih.gov/31509971/ ↩︎
Pimentel M, Leite G, Joo L. Real-world Study of Three-gas Breath Testing Nationwide and the Association With Symptoms. Journal of Clinical Gastroenterology. 2026. https://pubmed.ncbi.nlm.nih.gov/41671534/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Chedid V, Dhalla S, Clarke JO. Herbal therapy is equivalent to rifaximin for the treatment of small intestinal bacterial overgrowth. Global Advances in Health and Medicine. 2014. https://pubmed.ncbi.nlm.nih.gov/24891990/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Kariv R, Tiomny E, Grenshpon R. Low-dose naltreoxone for the treatment of irritable bowel syndrome: a pilot study. Digestive Diseases and Sciences. 2006. https://pubmed.ncbi.nlm.nih.gov/17080248/ ↩︎ ↩︎ ↩︎
Lazzini S, Polinelli W, Riva A. The effect of ginger (Zingiber officinalis) and artichoke (Cynara cardunculus) extract supplementation on gastric motility: a pilot randomized study in healthy volunteers. European Review for Medical and Pharmacological Sciences. 2016. https://pubmed.ncbi.nlm.nih.gov/26813467/ ↩︎ ↩︎ ↩︎ ↩︎
Giacosa A, Guido D, Grassi M. The Effect of Ginger (Zingiber officinalis) and Artichoke (Cynara cardunculus) Extract Supplementation on Functional Dyspepsia: A Randomised, Double-Blind, and Placebo-Controlled Clinical Trial. Evidence-Based Complementary and Alternative Medicine. 2015. https://pubmed.ncbi.nlm.nih.gov/25954317/ ↩︎ ↩︎
Cuffe MS, Staudacher HM, Aziz I. Efficacy of dietary interventions in irritable bowel syndrome: a systematic review and network meta-analysis. The Lancet Gastroenterology & Hepatology. 2025. https://pubmed.ncbi.nlm.nih.gov/40258374/ ↩︎
Chu P, He Y, Hu F. The effects of low FODMAP diet on gut microbiota regulation: A systematic review and meta-analysis. Journal of Food Science. 2025. https://pubmed.ncbi.nlm.nih.gov/40035292/ ↩︎ ↩︎ ↩︎
Bogdanowska-Charkiewicz D, Górski P, Jurkowska G. Effectiveness of the low FODMAP diet in patients with irritable bowel syndrome and small intestine bacterial overgrowth syndrome. Frontiers in Nutrition. 2026. https://pubmed.ncbi.nlm.nih.gov/41684777/ ↩︎ ↩︎