¶ Microscopic Colitis
| Primary Subtypes | Collagenous Colitis, Lymphocytic Colitis |
| Clinical Presentation | Chronic, Watery, Non-bloody Diarrhea |
| Endoscopy Finding | Normal or Near-Normal Mucosa |
| Primary Drug Triggers | NSAIDs, PPIs, SSRIs, Levodopa |
| First-Line Therapy | Oral Budesonide (9 mg/day) Taper |
| Demographics | Predominantly Females aged >60 |
Microscopic Colitis is a chronic inflammatory bowel disease characterized by chronic, high-volume, watery, non-bloody diarrhea with a macroscopically normal or near-normal colonic mucosa on colonoscopy. The diagnosis is established strictly through histopathological analysis of colonic mucosal biopsies, which differentiate the disease into two primary subtypes: Collagenous Colitis (CC) and Lymphocytic Colitis (LC)[1][2]. Frequently triggered or exacerbated by common pharmaceutical agents (such as PPIs, NSAIDs, and SSRIs), microscopic colitis yields to targeted, non-systemic corticosteroid therapy (Budesonide) and lifestyle adaptations, offering an excellent clinical prognosis without elevated risks of colorectal cancer[3][1:1][2:1].
¶ At a glance
Key points (high-level summary)
- Normal Endoscopy: The colon appears macroscopically healthy during colonoscopy; multiple random mucosal biopsies are mandatory to make the diagnosis[1:2][2:2].
- Primary Symptomatology: Characterized by sudden-onset, chronic, nocturnal, and voluminous watery diarrhea, accompanied by fecal urgency and abdominal cramps[1:3].
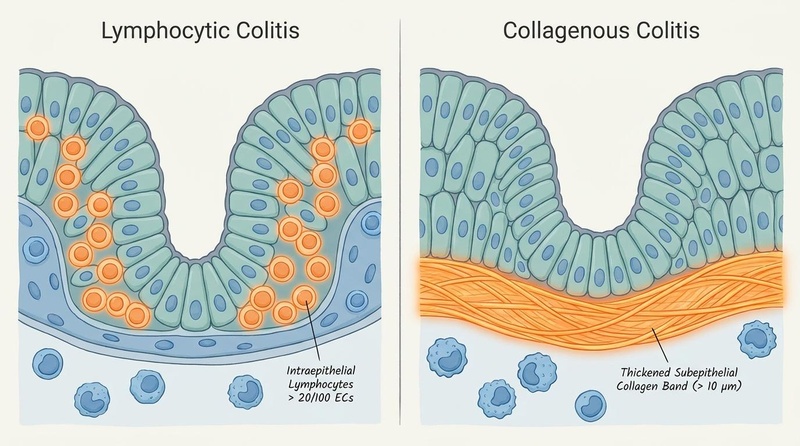
- Subtype Profiles: Collagenous Colitis features a thickened subepithelial collagen band, whereas Lymphocytic Colitis is defined by intense intraepithelial lymphocytic infiltration[2:3].
- Therapeutic Standard: Oral budesonide (9 mg/day) represents the gold-standard induction therapy, producing rapid clinical response and histological remission within 2–4 weeks[1:4].
What people use it for
- Aims: Complete resolution of chronic watery diarrhea, restoration of colonic fluid and electrolyte absorption, discontinuation of drug triggers, and maintenance of steroid-free clinical remission[1:5][2:4].
- Evidence quality: High-certainty evidence from multiple randomized controlled trials supports oral Budesonide; moderate-certainty evidence supports the identification of drug-induced etiologies and bile acid binders[3:1][1:6].
¶ What is Microscopic Colitis?
Microscopic Colitis is an underdiagnosed cause of chronic, non-infectious diarrhea that primarily compromises mucosal epithelial transport.
¶ Epidemiology and Age Predominance
The global incidence of microscopic colitis has risen significantly over the past three decades, primarily due to aging populations and widespread clinical awareness. It exhibits a distinct age and sex distribution, predominantly affecting individuals over the age of 60, with a striking female-to-male ratio of approximately 4:1 to 9:1 for Collagenous Colitis, and 2:1 to 4:1 for Lymphocytic Colitis[4]. While pediatric-onset microscopic colitis is exceptionally rare, it is occasionally diagnosed in children with concurrent celiac disease or autoimmune enteropathy[5].
¶ Clinical Presentation
The hallmark symptom of microscopic colitis is chronic, watery, non-bloody diarrhea. Stool volumes are frequently significant, ranging from 500 mL to over 2 liters per day, and are often accompanied by fecal urgency, fecal incontinence, nocturnal bowel movements, and crampy abdominal pain. Unlike classical IBD (Crohn's or UC), there is a notable absence of hematochezia (bloody stools), systemic fever, or progressive weight loss, although severe dehydration and electrolyte imbalances (hypokalemia) can occur in elderly patients[1:7].
¶ Subtypes and Drug-Induced Etiologies
Microscopic colitis is categorized into two histopathological patterns which share clinical symptoms but exhibit distinct microscopic structures:
¶ 1. Collagenous Colitis (CC)
Defined by a thickened, continuous subepithelial collagen band immediately beneath the epithelial basement membrane. While healthy colonic mucosa features a collagen layer of  µm, CC is diagnosed when the band thickness exceeds 10 µm. This collagenous deposition is frequently accompanied by epithelial cell damage (detachment of the epithelium from the basement membrane) and a moderate inflammatory infiltration of the lamina propria[2:5].
µm, CC is diagnosed when the band thickness exceeds 10 µm. This collagenous deposition is frequently accompanied by epithelial cell damage (detachment of the epithelium from the basement membrane) and a moderate inflammatory infiltration of the lamina propria[2:5].
¶ 2. Lymphocytic Colitis (LC)
Defined by a marked increase in intraepithelial lymphocytes (IELs) in the surface epithelium. LC is diagnosed when there are ≥20 intraepithelial lymphocytes per 100 epithelial cells (compared to <5 in a healthy colon). In LC, the subepithelial collagen band remains normal ( µm), but epithelial degeneration and lamina propria inflammation are prominent[2:6].
¶ The Role of Pharmaceutical Triggers
A key feature of microscopic colitis is its strong, established association with several widely prescribed medications. These agents are believed to disrupt epithelial tight junctions or alter mucosal metabolism:
- Non-Steroidal Anti-Inflammatory Drugs (NSAIDs): e.g., Ibuprofen, Diclofenac, Naproxen. NSAIDs inhibit cyclooxygenase (COX) enzymes, depleting mucosal prostaglandins and increasing mucosal permeability[3:2].
- Proton Pump Inhibitors (PPIs): e.g., Lansoprazole, Omeprazole, Esomeprazole. Lansoprazole carries the strongest clinical association with microscopic colitis flares[1:8].
- Selective Serotonin Reuptake Inhibitors (SSRIs): e.g., Sertraline, Fluoxetine, Escitalopram. Sertraline has been documented to trigger acute flares during pregnancy and in elderly cohorts[3:3][6].
- Levodopa/Carbidopa: Used in Parkinson's disease, levodopa is associated with drug-induced microscopic colitis that completely resolves upon transition to subcutaneous delivery systems[7][8].
¶ Diagnostic and Histopathological Framework
Because the colonic mucosa appears normal or near-normal during colonoscopy, making the diagnosis of microscopic colitis depends entirely on obtaining mucosal biopsies:
- Colonoscopy with Segmental Biopsies: Random biopsies must be obtained from multiple segments of the colon, including the ascending, transverse, descending, and sigmoid colon. This is critical because histopathological changes can be segmental and patchy; taking biopsies from the rectum alone can miss up to 20% of cases[1:9].
- Histopathological Criteria:
- Collagenous Colitis: Subepithelial collagen band >10 µm in thickness, stained with Masson's trichrome to clearly visualize collagen fibers, combined with epithelial cell flattening and lamina propria infiltration[2:7].
- Lymphocytic Colitis: Surface epithelial infiltration with ≥20 IELs per 100 epithelial cells, using CD3 immunohistochemistry to highlight T-lymphocytic structures if conventional H&E staining is inconclusive[2:8].
- Laboratory Testing to Rule Out Mimics: Patients should undergo screening for Celiac Disease (serum IgA anti-tissue transglutaminase) due to a strong immunological association, and stool testing to rule out Clostridioides difficile and other enteric pathogens[1:10].
¶ Evidence summary table (human outcomes)
| Target Indication | Intervention | Typical Effect Size | Certainty of Evidence | Primary Study Support | Clinical Notes |
|---|---|---|---|---|---|
| Induction of Clinical Remission | Oral Budesonide (9 mg/day) | High | Multi-Center RCTs[1:11][2:9] | Induces clinical response within 7–14 days; highly effective for both CC and LC. | |
| Maintenance of Clinical Remission | Low-dose Budesonide (3–6 mg/day) | High | Systematic Reviews[1:12] | Required in approximately 30–40% of patients who experience relapse after induction taper. | |
| Management of Drug-Induced MC | Discontinuation of offending drug (PPI, NSAID, SSRI) | Moderate | Observational Cohorts[3:4][1:13] | Leads to complete resolution of symptoms in up to 30% of drug-induced cases without steroids. | |
| Treatment of Concomitant Bile Acid Malabsorption | Bile Acid Sequesterants (Cholestyramine 4 g/day) | Moderate | Retrospective Studies[1:14] | Indicated for patients with concurrent bile acid diarrhea or those failing budesonide. | |
| Symptom Control in Mild MC | Loperamide or Bismuth Subsalicylate | Low | Clinical Cohorts[1:15] | Provides symptomatic relief of watery diarrhea; does not induce histological healing. | |
| Management of Refractory MC | Anti-TNF Biologics (Infliximab / Adalimumab) | Moderate | Case Series & Reviews[1:16] | Reserved for rare, severe, budesonide-refractory cases; induces rapid mucosal healing. |
¶ Pathophysiological Mechanisms
The pathogenesis of microscopic colitis involves a combination of genetic susceptibility, barrier dysfunction, and an abnormal mucosal immune response:
[ HLA-DQ2/DQ8 Genotype / Drug Exposure ]
│
▼
[ Epithelial Barrier Tight Junction Collapse ]
(Disrupted by NSAIDs, PPIs, or Luminal Toxins)
│
▼
[ Hyperosmolar Fluid Leakage ]
│
▼
[ Antigen Translocation & Presentation ]
│
┌────────────────────────┴────────────────────────┐
▼ ▼
[ Intraepithelial CD8+ T Cells ] [ Lamina Propria Activation ]
(Release Granzyme B & Perforin) (IL-1β, TNF-α, IFN-γ release)
│ │
▼ ▼
[ Epithelial Cell Apoptosis ] [ Myofibroblast Activation ]
│ │
│ ▼
│ [ Subepithelial Collagen Band ]
│ (Deposition of Type I & III)
│ │
└────────────────────────┬────────────────────────┘
▼
[ Severe Secretory Watery Diarrhea ]
- Genetic Predisposition and HLA Association: Microscopic colitis is strongly associated with the HLA-DQ2 and HLA-DQ8 haplotypes, sharing a genetic susceptibility pattern with celiac disease. This association suggests a common pathway of aberrant antigen presentation to CD4+ T-helper cells[1:17].
- Epithelial Barrier Dysfunction: Chronic exposure to drug triggers (such as PPIs or NSAIDs) alters luminal pH or inhibits mitochondrial respiration in colonocytes. This disrupts tight junction protein complexes (claudins, occludin), increasing mucosal permeability and allowing luminal antigens, bile acids, or bacteria to enter the lamina propria[9].
- T-Cell-Mediated Cytotoxicity: Surface epithelium is heavily infiltrated by cytotoxic CD8+ T lymphocytes expressing the integrin alpha-E beta-7 (CD103), which binds to E-cadherin on epithelial cells. These cytotoxic T cells release perforin and granzyme B, inducing epithelial cell apoptosis, flat enterocyte morphology, and desquamation.
- Bicarbonate/Chloride Exchanger Downregulation: The inflammatory cytokines TNF-alpha and IFN-gamma downregulate key transmembrane apical transporters, specifically the DRA (Downregulated in Adenoma / SLC26A3) Cl-/HCO3- exchanger. This blocks active sodium and chloride absorption, shifting the colonic mucosa from an absorptive state to an active secretory state, producing high-volume watery diarrhea.
- Pericryptal Fibrogenesis (in CC): In Collagenous Colitis, activated subepithelial myofibroblasts upregulate the synthesis of collagen types I and III in response to local TGF-beta 1 production. The resulting subepithelial collagen band acts as a physical barrier, further impeding water and sodium absorption[2:10].
¶ Therapeutic Protocols and Decision Paths
Clinical management focuses on withdrawing triggers, inducing remission with budesonide, and correcting fluid-electrolyte balances.
¶ Step 1: Trigger Elimination
Review the patient's medication list. Systematically discontinue suspected triggering agents:
- Discontinue all NSAIDs; substitute Acetaminophen for pain management.
- Discontinue lansoprazole and other PPIs; substitute H2-receptor antagonists (e.g., Famotidine) if acid suppression is mandatory.
- Evaluate SSRI indications; if sertraline is the suspected trigger, coordinate a taper and transition to an alternative antidepressant class (e.g., Bupropion).
¶ Step 2: First-Line Budesonide Induction
- Budesonide (Entocort EC / Ortikos): Initiate 9 mg orally once daily in the morning for 6 to 8 weeks.
- Taper Protocol: After 6 weeks of complete clinical resolution, initiate a gradual taper:
- 6 mg orally once daily for 2 weeks.
- 3 mg orally once daily for 2 weeks, then discontinue.
- Pharmacological Note: Budesonide is a high-potency corticosteroid with an oral formulation that utilizes an ethylcellulose-coated granule system. This delays release until the drug reaches the terminal ileum and colon. Because it undergoes extensive first-pass hepatic metabolism via the CYP3A4 enzyme (90% first-pass clearance), it delivers potent local anti-inflammatory effects with minimal systemic steroid adverse effects.
¶ Step 3: Management of Relapse and Refractory Disease
- Budesonide Maintenance: Approximately 30–40% of patients experience symptomatic relapse within 6 months of discontinuing budesonide. In these patients, re-induce with 9 mg/day and establish the lowest effective maintenance dose (typically 3 mg to 6 mg orally once daily)[1:18].
- Bile Acid Sequesterants: If budesonide is contraindicated or fails, initiate Cholestyramine (4 g orally 1 to 3 times daily). Cholestyramine binds luminal bile acids, preventing bile-acid-induced colonic secretion which coexists in up to 40% of microscopic colitis patients[1:19].
- Anti-TNF Therapy: In rare, severe, budesonide-refractory cases, initiate Infliximab (5 mg/kg IV induction) to downregulate TNF-alpha and achieve rapid clinical and histological remission[1:20].
¶ Safety, Toxicology, and Clinical Monitoring
Despite the localized delivery of budesonide, long-term safety monitoring is required, particularly in elderly populations:
¶ Serious Adverse Events & Adverse Reactions
- Drug-Drug Interactions (CYP3A4): Budesonide is metabolized primarily by the cytochrome P450 3A4 enzyme. Concomitant administration of strong CYP3A4 inhibitors (e.g., Ketoconazole, Itraconazole, Ritonavir, or Grapefruit juice) can dramatically increase systemic budesonide exposure, leading to Cushingoid side effects (fluid retention, moon face, striae).
- Bone Mineral Density (BMD) Loss: Chronic use of budesonide (>6 months), even at maintenance doses of 3–6 mg/day, can accelerate bone resorption. Perform baseline and follow-up dual-energy X-ray absorptiometry (DEXA) scans, and supplement patients with calcium (1,200 mg/day) and Vitamin D3 (2,000 IU/day).
- Glaucoma and Cataracts: Long-term steroid therapy can increase intraocular pressure. Perform annual ophthalmological screening in patients on chronic budesonide.
¶ Clinical Monitoring Protocol
┌────────────────────────────────────────────────────────┐
│ DIAGNOSIS & BUDESONIDE START │
│ - Confirm diagnosis via Segmental Biopsies │
│ - Discontinue NSAIDs, PPIs, and Sertraline │
│ - Start Budesonide 9 mg/day; supplement Ca & Vit D3 │
└───────────────────────────┬────────────────────────────┘
│
▼
┌────────────────────────────────────────────────────────┐
│ WEEK 4 EVALUATION │
│ - Confirm clinical response (<3 stools/day, formed) │
│ - Monitor electrolytes (potassium) if elderly │
│ - Check for CYP3A4 drug-drug interactions │
└───────────────────────────┬────────────────────────────┘
│
▼
┌────────────────────────────────────────────────────────┐
│ WEEK 8 TAPER START │
│ - Initiate Budesonide Taper (6 mg -> 3 mg -> Stop) │
│ - If relapse occurs: return to lowest effective dose │
│ - If budget/side-effects limit Budesonide: add │
│ Cholestyramine 4 g/day or Bismuth Subsalicylate │
└───────────────────────────┬────────────────────────────┘
│
▼
┌────────────────────────────────────────────────────────┐
│ LONG-TERM SURVEILLANCE │
│ - If on chronic Budesonide: annual DEXA scan and │
│ Ophthalmological exam │
│ - Re-biopsy only if symptoms recur or fail to respond │
└────────────────────────────────────────────────────────┘
¶ Practical FAQ
Does Microscopic Colitis increase the risk of Colorectal Cancer?
No. Extensive long-term epidemiological cohort studies have conclusively shown that patients with microscopic colitis do not have an increased risk of developing colorectal cancer or colonic dysplasia compared to the general population. Consequently, routine colonoscopic cancer surveillance is not required for microscopic colitis, unlike ulcerative colitis or Crohn's disease[1:21][2:11].
What is the association between Microscopic Colitis and Celiac Disease?
There is a strong immunological and genetic association between microscopic colitis and celiac disease, driven by shared HLA-DQ2/DQ8 haplotypes. Approximately 2–10% of patients with microscopic colitis have biopsy-proven celiac disease, and microscopic colitis is a leading cause of "refractory" watery diarrhea in celiac patients who are otherwise adherent to a gluten-free diet. Screening with anti-tTG IgA is recommended[1:22].
Is Bismuth Subsalicylate effective for treating Microscopic Colitis?
Yes, in mild cases. High-dose Bismuth Subsalicylate (e.g., eight 262 mg tablets orally daily in divided doses for 8 weeks) has been shown in small clinical trials to induce clinical response and improve mucosal histopathology in patients with microscopic colitis. It acts via its anti-secretory, anti-inflammatory, and anti-bacterial properties. However, its use is limited by compliance (pill burden) and the risk of bismuth toxicity with prolonged administration.
Can Microscopic Colitis resolve spontaneously without any treatment?
Yes. Spontaneous clinical remission has been documented in up to 15–20% of patients with microscopic colitis. This is particularly common in drug-induced cases where the offending medication (such as an NSAID or PPI) is successfully identified and permanently discontinued, allowing the colonic mucosal barrier to restore itself without medical intervention[3:5][1:23].
¶ Methods
This monograph was synthesized by conducting a systematic review of consensus guidelines published by the American Gastroenterological Association (AGA) and the European Microscopic Colitis Group (EMCG), combined with multi-center clinical trials and systematic reviews up to July 2026. Evidence quality was assessed using the GRADE framework.
¶ References
¶ Update Log
- 2026-07-07: Clinical monograph created, detailing lymphocytic and collagenous subcategories of microscopic colitis, identifying critical pharmaceutical triggers, and providing oral Budesonide induction protocols.
Singh P, Lee A, Sheth NM. Chronic, Noninfectious Diarrhea: A Review. JAMA. 2026. https://pubmed.ncbi.nlm.nih.gov/41770539/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Ghoneim S, Drage MG, Burke KE. Microscopic Colitis: Evidence-Based Guide to Diagnosis and Management. Annual review of medicine. 2026. https://pubmed.ncbi.nlm.nih.gov/41592927/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Saraga A, Bocchino R, Gade A. Sertraline-Associated Microscopic Colitis Flare in Pregnancy. ACG case reports journal. 2026. https://pubmed.ncbi.nlm.nih.gov/42041026/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Yu HJ, Kim S, Oh J. Global Incidence, Prevalence, and Risk Factors of Microscopic Colitis, 1984-2020: A Systematic Review and Meta-Analysis. Clinical gastroenterology and hepatology. 2026. https://pubmed.ncbi.nlm.nih.gov/41985775/ ↩︎
Hernández Díaz LM, Hasan B, Almallouhi A. Microscopic colitis in children: A single-center experience and systematic review. Journal of pediatric gastroenterology and nutrition. 2026. https://pubmed.ncbi.nlm.nih.gov/41930668/ ↩︎
Gerbier E, Abolhassani N, Dupuis M. Use of medications to treat inflammatory bowel diseases before and during pregnancy in Switzerland between 2012 and 2019: an observational study using the claims-based MAMA cohort. BMC gastroenterology. 2026. https://pubmed.ncbi.nlm.nih.gov/42277663/ ↩︎
Macht A, Cathomas G, Bauer E. Chronic diarrhea in Parkinson's disease during Levodopa therapy. Praxis. 2026. https://pubmed.ncbi.nlm.nih.gov/42200385/ ↩︎
Hintner R, Eberhardt F, Kofler M. Resolution of Levodopa/Dopa-Decarboxylase Inhibitor-Associated Microscopic Colitis with Subcutaneous Foslevodopa/Foscarbidopa: A Case Series and Review of the Literature. Movement disorders clinical practice. 2026. https://pubmed.ncbi.nlm.nih.gov/41668674/ ↩︎
Khasanov R, Boettcher M, Wessel LM. All roads lead to NF-κB: the NF-κB pathway as a major target for intestinal inflammatory disorders. Frontiers in immunology. 2026. https://pubmed.ncbi.nlm.nih.gov/42148126/ ↩︎