¶ Older Adult Longevity and Function
| Parameter | Clinical Target & Strategy | Evidence Certainty |
|---|---|---|
| Primary Goal | Preservation of independent activities of daily living (ADLs) and prevention of frailty. | High (Consensus) |
| Skeletal Muscle | >80% 1RM Heavy Resistance Training + Power-focused Concentric Accents [1][2] | High (GRADE: High) |
| Postural Control | Perturbation-Based Balance Training (PBBT) + Multisensory Reweighting [3][4] | High (GRADE: High) |
| Protein Nutrition | 1.2–2.0 g/kg/day with $\ge$30g per meal containing $\ge$3g Leucine [5][6] | High (GRADE: High) |
| Sleep Quality | CBT-I (first-line) + 2 mg Prolonged-Release Melatonin [7][8][9] | High (GRADE: High) |
| Cognitive Reserve | Autophagy upregulation (Spermidine), Cholinergic (Alpha-GPC), Somatotrophic (GHRH) [10][11][12] | Moderate (GRADE: Moderate) |
| Social Health | Cognitive-behavioral reduction of loneliness + Eudaimonic Purpose [13][14][15] | High (GRADE: High) |
| Medication Safety | Polypharmacy reduction, Beers Criteria screening, and CNS-active deprescribing [16][17][9:1] | High (GRADE: High) |
| Frailty Intervention | Lomecel-B (Laromestrocel) Allogeneic Mesenchymal Stem Cell IV Infusion [18] | Moderate (GRADE: Moderate) |
¶ Safety "Traffic Light" Matrix
CRITICAL CLINICAL BOUNDARIES
- RED LIGHT (Absolute Contraindications): Progressive resistance training is contraindicated in unstabilized acute spinal fractures, acute myocardial infarction within 6 weeks, or severe uncompensated heart failure. Dynamic, unharnessed perturbation balance training is prohibited in patients with severe cerebellar ataxia or untreated high-risk carotid stenosis.
- YELLOW LIGHT (Precautions & Modifications): High-load impact or high-velocity training must be modified to closed-chain, low-impact movements in cases of advanced bone mineral density loss (T-score < -3.0). Prolonged-release melatonin should be monitored in patients taking oral anticoagulants.
- GREEN LIGHT (Fully Cleared): Supervised progressive heavy resistance loading, high-density protein supplementation, cognitive behavioral therapy for insomnia (CBT-I), and structured eudaimonic social integration are safe, recommended, and clinically verified for both healthy and frail older adult populations.
¶ Intervention Bottom Line
To successfully preserve functional independence and cognitive longevity after age 60, clinical programming must move beyond passive "maintenance" models and shift toward targeted, high-threshold stimulus. Reversing age-related decline requires high-load mechanical tension to overcome motor unit denervation [1:1][2:1], elevated per-meal amino acid thresholds to defeat anabolic resistance [5:1][6:1], active sensory reweighting to prevent falls [3:1][4:1], and systematic reduction of polypharmacy [17:1].
¶ 2. Contextual Narrative
¶ The "Why": Benefits of targeted clinical programming
Functional aging is defined not merely by the absence of disease, but by the preservation of physiological reserve. Between the ages of 60 and 80, individuals lose up to 50% of their fast-twitch motor units, leading to a catastrophic decline in muscle power that outpaces muscle mass loss by a factor of three [2:2]. This drop in rate of force development (RFD) is the primary driver of fall susceptibility and subsequent institutionalization. By initiating targeted progressive heavy resistance training, dynamic neuromuscular conditioning, and anabolic protein partitioning, older adults can actively reverse osteosarcopenic pathways, restore hippocampal sleep-dependent memory consolidation, and repress systemic pro-inflammatory gene transcription [1:2][7:1][19][15:1].
¶ Clinical Segmentation of Target Populations
¶ Healthy Older Adults (Aged 60+)
- Goal: Maximize cognitive reserve, sustain peak skeletal power, and preserve musculoskeletal health.
- Strategy: Heavy resistance training (>80% 1RM) twice weekly, high-dose leucine-rich protein distribution, and advanced cognitive challenges (e.g., dual-task navigation).
¶ Frail Adults & Sarcopenia/Osteosarcopenia Cohorts
- Goal: Reclaim basic functional capacity (e.g., floor transfers, chair rises), increase femoral bone mineral density, and lower systematic chronic inflammation (inflammaging).
- Strategy: Multi-component Falls Management Exercise (FaME) programming [20], supervised closed-chain progressive resistance training, combined synergistic Vitamin D3/K2 supplementation [21], and clinical evaluation for allogeneic mesenchymal stem cell therapy (Lomecel-B) [18:1].
¶ Individuals Rebuilding after Prolonged Inactivity
- Goal: Safe, graduated motor unit re-recruitment, re-establishment of kinetic chain integrity, and alleviation of the "fear of falling" (FoF).
- Strategy: Low-to-moderate intensity progressive resistance loading, static-to-dynamic transition balance protocols (FallProof program) [22], and progressive sensory reweighting exercises to restore spatial orientation under fluctuating environmental conditions [4:2].
¶ Patients with Controlled Chronic Illness
- Goal: Improve healthspan and functional capacity while respecting specific metabolic, cardiovascular, or arthritic limits.
- Strategy: Tailored training volumes with careful hemodynamic monitoring. For cardiovascular disease, avoid prolonged Valsalva maneuvers by implementing controlled, rhythmic breathing during eccentric phases of lifting.
¶ Sex-Specific Considerations
- Postmenopausal Women: Rapid estrogen decline triggers osteoclastic acceleration. Resistance training must emphasize high-load mechanical forces (>80% 1RM) and axial loading (e.g., supervised deadlifts, squats) to increase femoral and lumbar bone mineral density, combined with activated calcium-regulatory agents (Vitamin D3 + Vitamin K2) [19:1][21:1].
- Older Men: Decline in bioavailable testosterone accelerates visceral adiposity and sarcopenic muscle loss. Clinical protocols must focus on maximizing muscle protein synthesis (MPS) via high-density essential amino acid boluses [5:2] and heavy multi-joint compound resistance training [2:3].
¶ 3. Practical Integration Protocols
Practical Daily, Weekly, and Monthly Clinical Protocols
¶ Daily Protocol: Anabolic Spiking, Sleep Alignment, and Cognitive Resilience
- 08:00 (Breakfast): High-density protein bolus (35–40g of whey protein or essential amino acid equivalent) containing $\ge$3g of Leucine to overcome the anabolic resistance threshold [5:3][6:2].
- 08:30 (Neuro-Cognitive Support): 300–600 mg of oral Alpha-GPC to provide bioavailable free choline for central cholinergic transmission [12:1].
- 10:00 (Sensory Integration): 10 minutes of sensory reweighting drills (e.g., standing on foam with eyes open/closed) [4:3].
- 13:00 (Lunch): High-density protein bolus (30–40g protein) [6:3].
- 19:00 (Dinner): Light protein intake (25–30g) paired with complex carbohydrates.
- 21:30 (Sleep Initiation): Cognitive Behavioral Therapy for Insomnia (CBT-I) progressive muscle relaxation session [7:2] + 2 mg Prolonged-Release Melatonin to restore endogenous slow-wave sleep architecture [8:1].
¶ Weekly Protocol: Neuromuscular Power and Balance Development
- Day 1 (Heavy Strength & Power Preservation):
- Dynamic Warm-up: 5 minutes of low-intensity walking + joint mobility.
- Compound Lifting: 3 sets of 5 repetitions of supervised Leg Press or Hack Squat at 80% 1RM. Concentrate on explosive, rapid concentric execution (concentric speed accent) followed by a controlled 3-second eccentric phase to target Type II fast-twitch muscle fibers [2:4].
- Upper Body Compound: 3 sets of 8 repetitions of seated chest press and cable rows at 70–75% 1RM.
- Floor-Transfer Drills: 2 reps of assisted or unassisted floor-to-standing transfers (essential survival skill to mitigate the "long lie" post-fall) [20:1].
- Day 2 (Postural Perturbation & Balance Conditioning):
- Perturbation Drills: 15 minutes of Perturbation-Based Balance Training (PBBT) utilizing rapid, unpredictable physical displacements (e.g., nudge challenges, manual perturbations by a trainer, or sliding balance platform work) [3:2].
- Multisensory Integration: 15 minutes of unstable surface navigation (foam pads, balance beams) with visual tracking tasks (catching a ball, head rotations) to drive sensory reweighting [4:4].
- Day 3 (Active Recovery & Social-Purpose Integration):
- Day 4 (Heavy Strength & Power Preservation): Repeat Day 1 programming with secondary compound exercises (e.g., chest flyes, lat pulldowns, knee extensions).
¶ Monthly Protocol: Medication, Biomarker, and Functional Assessment
- Week 1 (Medication & Deprescribing Review): Cross-reference all medications against the AGS Beers Criteria [17:2]. Under clinical supervision, begin a gradual tapering program for any non-essential central nervous system (CNS)-active medications (such as benzodiazepines or Z-drugs), substituting with non-pharmacological CBT-I [9:2].
- Week 2 (Functional Assessment): Perform standardized physical function monitoring:
- Timed Up and Go (TUG) Test: Target performance of <10 seconds.
- Short Physical Performance Battery (SPPB): Target score of 11–12 points.
- 30-Second Chair Stand Test: Quantify lower limb power.
- Week 4 (Biomarker and Cognitive Tracking): Evaluate subjective sleep quality (via Pittsburgh Sleep Quality Index, PSQI), cognitive clarity (via Montreal Cognitive Assessment, MoCA, if indicated), and review monthly adherence to eudaimonic social integration goals.
4. Mechanisms of Physiological Aging
¶ 1. Neuromuscular Motor Unit Denervation and Power Loss
The loss of muscular capacity in older adults is primarily a neural event rather than a purely muscular one. Beginning around age 60, there is a progressive apoptosis of alpha motor neurons in the anterior horn of the spinal cord. This results in the denervation of entire motor units, specifically targeting the high-threshold Type II (fast-twitch, glycolytic) fibers. While some Type II fibers are rescued by re-innervation from nearby slow-twitch (Type I) motor units, this process results in giant, slow-conducting motor units with impaired Rate of Force Development (RFD). Heavy resistance training (>80% 1RM) provides the high-threshold electrical stimulus necessary to recruit remaining fast-twitch units, restoring neuromuscular power and protecting against dynamic slips or trips [1:3][2:5].
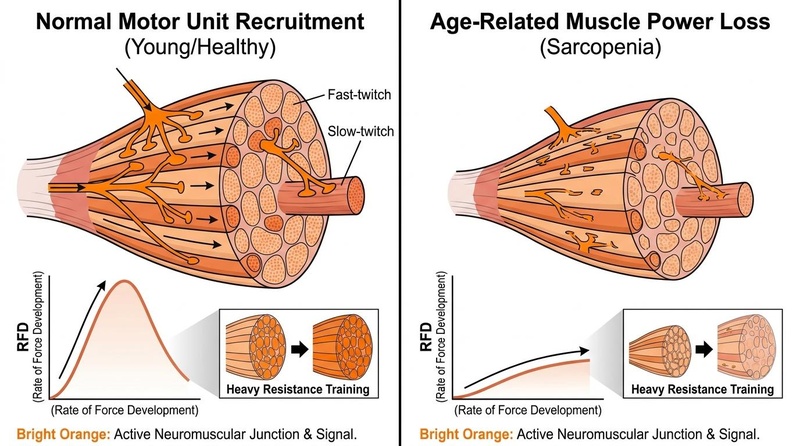
Figure 1: Neuromuscular Motor Unit Recruitment and Power Preservation. Heavy resistance training (>80% 1RM) rescues fast-twitch (Type II) fibers and restores rate of force development (RFD).
¶ 2. Postural Instability and Multisensory Reweighting Deficits
Maintaining upright posture is a complex neurological process requiring the integration of three primary sensory streams: visual, vestibular, and proprioceptive (somatosensory). Healthy nervous systems continuously perform "sensory reweighting"—shifting the priority of these streams depending on environmental demands (e.g., relying heavily on vestibular and proprioceptive inputs when walking in a dark room).
In older adults, sensory receptor density declines (e.g., loss of vestibular hair cells, pacinian corpuscles in the soles of the feet), and central processing slows down. The brain becomes unable to dynamically reweight inputs fast enough, leading to dynamic center-of-pressure (CoP) sway and falls during sudden sensory or physical perturbations. Perturbation-Based Balance Training (PBBT) forces rapid spinal-level motor adaptations and accelerates sensory reweighting processing in the central nervous system [3:3][4:5] (see also Balance Training).
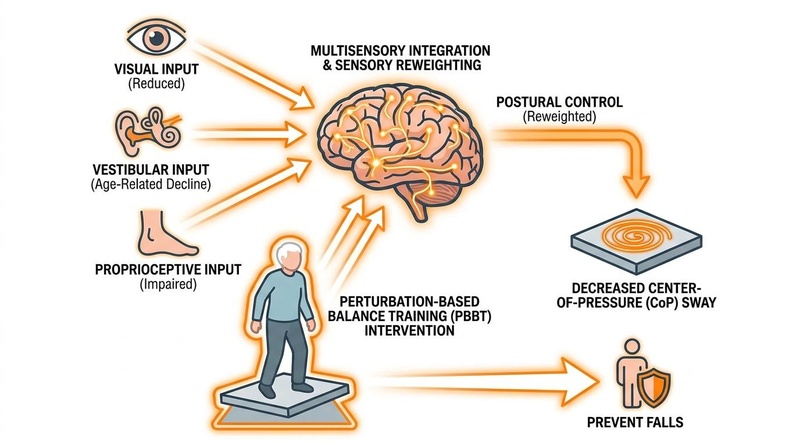
Figure 2: Multisensory Integration and Sensory Reweighting in Postural Control. Perturbation-based training (PBBT) improves the central nervous system's capacity to dynamically prioritize stable sensory inputs.
¶ 3. Anabolic Resistance and Skeletal Sarcopenia
Anabolic resistance is the blunted skeletal muscle protein synthesis (MPS) response to normal physiological concentrations of dietary amino acids and mechanical loading. In young muscle, a small dose of protein (10–15g) is sufficient to increase intracellular leucine levels, open the LAT1 amino acid transporter, activate the mechanistic target of rapamycin complex 1 (mTORC1) pathway, and trigger MPS.
In older muscle, age-related inflammation, capillary density loss, and ribosomal deconditioning raise the threshold required to activate mTORC1. When an older adult consumes a sub-threshold protein meal (e.g., a standard 15g breakfast), the anabolic machinery remains inactive, leading to a net negative daily nitrogen balance and progressive sarcopenia. Overcoming this barrier requires consuming high-density, leucine-rich protein boluses ($\ge$30–40g of protein providing $\ge$3g of free leucine) [5:4][6:4] (see also Protein).
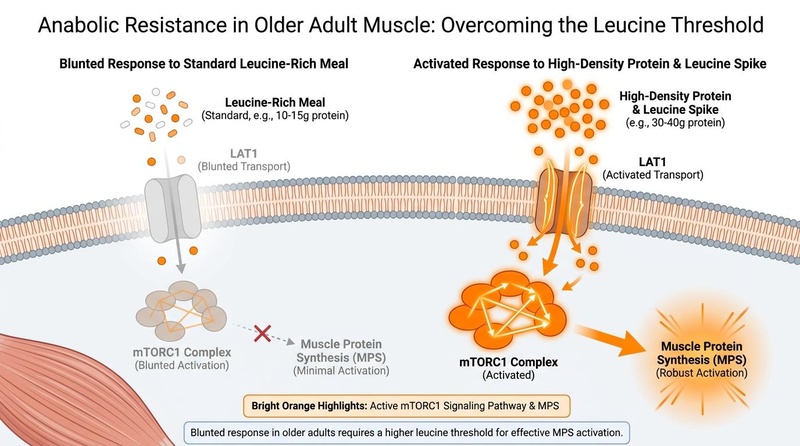
Figure 3: Overcoming Anabolic Resistance. Aging muscle cells require higher per-meal leucine concentrations (~3g) to robustly activate the LAT1/mTORC1 pathway and trigger muscle protein synthesis (MPS).
¶ 4. Sleep Architecture Decay and Slow-Wave Restructuring
Aging is accompanied by a dramatic fragmentation of sleep architecture, characterized by a progressive loss of Slow Wave Sleep (SWS; N3 stage) and a reduction in slow-wave activity (SWA; 0.5–4.5 Hz oscillations). SWA is the physiological driver of synaptic pruning and sleep-dependent memory consolidation. It also coordinates the glymphatic system, which clears neurotoxic amyloid-beta and tau aggregates from brain tissues.
The decline in slow-wave activity is linked to atrophy of the prefrontal cortex and age-related calcification of the pineal gland, which blunts nocturnal melatonin secretion. Substituting pharmacological sedatives (which suppress SWA) with Cognitive Behavioral Therapy for Insomnia (CBT-I) and prolonged-release melatonin actively restores slow-wave sleep duration and enhances memory retention [7:3][8:2][9:3].
¶ 5. Psychoneuroimmunology: The CTRA Pathway in Loneliness
Subjective loneliness and social isolation are not merely emotional states; they represent profound physiological stressors. Chronically lonely older adults exhibit a sustained activation of the sympathetic nervous system (SNS) and the hypothalamic-pituitary-adrenal (HPA) axis. This sustained neuroendocrine signaling alters gene transcription within circulating leukocytes, initiating a molecular profile known as the Conserved Transcriptional Response to Adversity (CTRA).
The CTRA is characterized by a systemic upregulation of pro-inflammatory genes (e.g., IL-1B, IL-6, TNF) and a concurrent downregulation of genes involved in type-1 interferon antiviral responses and antibody synthesis. Cultivating a strong sense of purpose in life (eudaimonic well-being) through structured social engagement reverses this transcriptional adversity profile, reduces epigenetic age (GrimAge), and suppresses chronic systemic inflammaging [14:2][15:3].
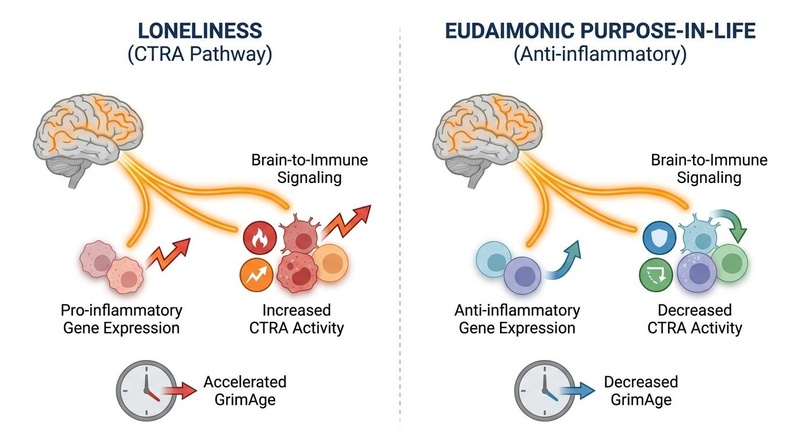
Figure 4: Neuro-Immune Axis and Eudaimonic Purpose. Subjective loneliness triggers the Conserved Transcriptional Response to Adversity (CTRA), whereas a strong sense of purpose in life reduces epigenetic age (GrimAge) and suppresses pro-inflammatory genes.
¶ 5. Evidence & Human Clinical Outcomes
¶ Human Effect Matrix
| Outcome | Interventions Evaluated | Efficacy / Absolute Effect Size | Certainty (GRADE) | Supported Study Types | Key Findings & Citations |
|---|---|---|---|---|---|
| Sarcopenia & Muscle Power | Heavy Resistance Training ( 1RM) vs. Traditional Lifting [1:4][2:6] | High | 1 Meta-Analysis, Multiple RCTs | Progressive high-load mechanical tension overcomes denervation-induced Type II fast-twitch muscle fiber decay [1:5][2:7]. | |
| Fall Prevention | Perturbation-Based Balance Training (PBBT) vs. Static Training [3:4][4:6] | High | 1 Systematic Review, 1 Meta-Analysis | PBBT forces spinal-level motor adaptations and accelerates sensory reweighting under environmental instability [3:5][4:7]. | |
| Community Fall Mitigation | Falls Management Exercise (FaME) Multi-Component Program [20:2][22:1] | High | 1 Scoping Review, 1 Systematic Review | Standardized multi-component training including floor-transfer drills significantly reduces dynamic instability [20:3][22:2]. | |
| Osteosarcopenia Bone Reclaiming | Supervised Resistance Training + High Impact Axial Loading [23][19:2] | High | 1 Systematic Review, 1 RCT (ERTO-K Trial) | High-load mechanical force stimulates osteoblastogenesis, promoting osteo-skeletal structural restoration [23:1][19:3]. | |
| Autophagy & Synaptic Repair | Oral Spermidine Supplementation (1.2 mg/day) [10:1][24] | Moderate | 1 Systematic Review, 1 Phase II RCT (SmartAge Trial) | Autophagic clearance of toxic amyloid-beta and tau aggregates maintains hippocampal neural integrity [10:2][24:1]. | |
| Executive & Memory Recovery | Growth Hormone-Releasing Hormone (GHRH, Tesamorelin 1mg/day) [11:1] | Moderate | Double-Blind, Placebo-Controlled RCT | GHRH administration increases systemic IGF-1 levels, promoting cortical synaptogenesis and neural plasticity [11:2]. | |
| Cognitive Score & Memory Restoration | Oral Choline Alfoscerate (Alpha-GPC) [12:2] | Moderate | Multiple Clinical RCTs | Alpha-GPC crosses the blood-brain barrier to upregulate acetylcholine synthesis, preventing transmission decay [12:3]. | |
| Slow-Wave Sleep Restoration | Cognitive Behavioral Therapy for Insomnia (CBT-I) + PR Melatonin [7:4][8:3] | High | Multiple RCTs | CBT-I combined with prolonged-release melatonin avoids sedative-hypnotic dependency and restores natural sleep architecture [7:5][8:4] (see also Sleep Optimization). | |
| Inflammatory Profile Remodeling | Cognitive Behavioral Therapy (CBT) for Loneliness + Purpose-in-Life [13:1][14:3][15:4] | High | 1 Meta-Analysis, 1 Transcriptomics Cohort, 1 Longitudinal Cohort | Solving perceived loneliness reverses systemic psychoneuroimmunological stress, decelerating biological aging [13:2][14:4][15:5]. | |
| Aging Frailty Musculoskeletal Rebirth | Allogeneic Mesenchymal Stem Cell IV Infusion (Lomecel-B / Laromestrocel) [18:2] | Moderate | Phase 2b Dose-Escalation RCT | Single IV infusion of Laromestrocel demonstrates profound anti-inflammatory activity, reversing physical frailty [18:3]. |
¶ 6. Comprehensive Safety, Toxicology, and Medication Management
¶ Polypharmacy, Beers Criteria, and CNS Deprescribing
As the human body ages, pharmacokinetic and pharmacodynamic profiles undergo dramatic shifts. Hepatic blood flow decreases by 30–40%, and glomerular filtration rate (GFR) drops progressively, leading to prolonged drug half-lives and an accumulation of drug metabolites. Polypharmacy (defined as the concurrent use of $\ge$5 medications) represents a major independent risk factor for cognitive decline, gait instability, and severe falls.
The American Geriatrics Society (AGS) Beers Criteria lists potentially inappropriate medications (PIMs) that must be avoided or carefully restricted in older adults [17:3]. Central nervous system (CNS)-active agents, including benzodiazepines (e.g., alprazolam, diazepam), non-benzodiazepine sedative-hypnotics ("Z-drugs" like zolpidem), tricyclic antidepressants (e.g., amitriptyline), and atypical antipsychotics, pose the highest hazard [16:1]. These agents induce motor and cognitive deconditioning, leading to a 1.5- to 2.4-fold increase in fall incidence [16:2].
Under strict clinical supervision, these drugs should be slowly tapered and replaced with non-pharmacological interventions, such as CBT-I for insomnia [9:4] and cognitive-behavioral therapies for anxiety or social distress [13:3].
¶ Cardiovascular, Hepatic, and Renal Monitoring
- CYP450 Metabolism: Aging alters the activity of major cytochrome P450 enzymes (particularly the CYP3A4 and CYP2D6 pathways). Co-administration of multiple substrates can cause massive spikes in serum concentrations, leading to toxicity.
- Renal Clearance: Dosage of water-soluble compounds and medications must be scaled according to estimated creatinine clearance (eGFR), utilizing the Cockcroft-Gault formula rather than serum creatinine alone, to prevent systemic toxicity.
- Hemodynamic Safety: Progressive exercise protocols must be modified in the presence of uncompensated orthostatic hypotension (defined as a drop in systolic blood pressure of $\ge$20 mmHg or diastolic blood pressure of $\ge$10 mmHg within 3 minutes of standing). Rhythmic, paced breathing during mechanical loading is mandatory to prevent unsafe intra-thoracic pressure spikes.
¶ 7. Clinician-Caregiver Coordination and Medical Boundaries
¶ Standard of Care Boundaries
This guide serves as an educational and clinical reference to optimize functional healthspan. However, clear boundaries exist between lifestyle/preventative modifications and acute medical management. Caregivers and fitness professionals must respect the limits of their practice:
- Exercise Modification: If an older adult presents with sudden, unilateral joint swelling, acute chest tightness, or unprovoked dyspnea, exercise must be suspended immediately.
- Bone Health: Preventive exercise (axial loading) is a long-term strategy. It does not replace medical pharmacological therapies (such as bisphosphonates, denosumab, or teriparatide) in patients diagnosed with severe osteoporosis at high risk for imminent fragility fractures.
- Cognitive Decline: Subjective cognitive decline or mild cognitive impairment may be supported with nutritional, cholinergic, or somatotrophic interventions [10:3][11:3][12:4]. However, rapid, progressive cognitive changes require formal diagnostic screening to rule out secondary, treatable etiologies (such as B12 deficiency, subdural hematoma, or severe hypothyroidism; see Cognitive Decline).
- Stem Cell Interventions: Emerging therapies such as Lomecel-B/Laromestrocel show exceptional efficacy in reversing frailty and downregulating systemic inflammation [18:4]. However, these are advanced investigational medical therapies that must be administered strictly within registered clinical trials or under approved expanded-access regulatory pathways.
¶ 8. Clinical Decision Tree
¶ 9. Comparative Intervention Analysis
| Intervention Modality | Primary Physiological Target | Rate of Force Development (RFD) Impact | Fall Risk Reduction | Musculoskeletal Safety Profile | Primary Limitations |
|---|---|---|---|---|---|
| Heavy Resistance Training ( 1RM) | Fast-twitch Type II myofiber hypertrophy, motor unit recruitment, osteogenesis. [1:6][2:8] | High | High (indirect via power recovery) | Moderate (Requires precise form; risk of joint strain if unsupervised) | Requires high cognitive engagement and qualified supervision. |
| Perturbation-Based Balance Training (PBBT) | Sensory reweighting, spinal reflex acceleration, reactive stepping latency reduction. [3:6][4:8] | Moderate | Extreme (Direct neuromuscular prevention) | High (Safe when conducted in a harness environment) | Highly dependent on specialized equipment or physical therapist guidance. |
| Static Balance Training (e.g., Tai Chi) | Proprioceptive feedback, slow-velocity control, core activation. [22:3] | None/Low | Moderate | Very High (Virtually zero injury risk) | Fails to condition rapid neuromuscular reflex pathways required during sudden slips. |
| Low-Load Resistance Training ( 1RM) | Muscle endurance, local metabolic vascularization. [19:4] | Low | Low (Minimal effect on dynamic fast-twitch recruitment) | Very High (Low joint stress) | Fails to stimulate significant myofibrillar hypertrophy or bone mineral density accrual. |
¶ 10. Practical FAQ
Why is walking alone insufficient to prevent muscle loss and falls?
Walking (low-intensity aerobic exercise) does not provide the mechanical tension required to recruit high-threshold Type II (fast-twitch) motor units, which are the first to degenerate during aging [2:9]. To reclaim the dynamic muscle power and rapid reflex recovery needed to catch oneself during a slip, older adults must engage in heavy resistance training and dynamic perturbation exercises that force the nervous system to recruit fast-twitch muscle fibers [1:7][3:7].
How do I know if my daily protein intake is actually preventing sarcopenia?
Simply hitting a total daily protein target is insufficient because of age-related "anabolic resistance" [5:5]. To trigger muscle protein synthesis (MPS), you must reach an "anabolic threshold" in a single meal by consuming at least 30–40g of high-quality protein containing approximately 3g or more of the amino acid Leucine [6:5]. Spreading protein evenly across breakfast, lunch, and dinner to ensure you hit this threshold at multiple points in the day is the most effective way to sustain muscle mass [6:6].
What is the Beers Criteria, and why is it important for fall prevention?
The Beers Criteria is a standardized list of medications maintained by the American Geriatrics Society that are potentially inappropriate for older adults [17:4]. Many common medications—especially sleeping pills, benzodiazepines, and certain antidepressants—act on the central nervous system, causing dizziness, slowed reflexes, and impaired balance, which increases fall risk by 1.5 to 2.4 times [16:3]. Reviewing your medications against this list and coordinating with a physician to taper off high-risk drugs is one of the most powerful ways to prevent falls [9:5].
Can older adults really safe-lift heavy weights above 80% of their maximum capacity?
Yes. Clinical trials consistently show that progressive heavy resistance training ( of 1-repetition maximum) is exceptionally well-tolerated and safe for adults aged 60 and older, including those with osteosarcopenia, when properly supervised [1:8][2:10]. Heavy lifting is highly effective for rapidly restoring spinal motor unit recruitment, increasing muscle size, and reversing bone density loss [2:11][19:5] (see also Strength Training).
How does having a strong "sense of purpose" affect physical longevity?
A high sense of purpose in life (eudaimonic well-being) acts as a physical buffer against biological aging. Lonely older adults experience a molecular stress response called the Conserved Transcriptional Response to Adversity (CTRA), which upregulates inflammatory genes and damages the immune system [15:6]. Cultivating strong social connections and a clear daily purpose suppresses this pro-inflammatory response, lowers systemic inflammation (inflammaging), and significantly decelerates epigenetic aging (GrimAge) [14:5][15:7].
¶ 11. Glossary
- Anabolic Resistance: The age-related blunting of skeletal muscle protein synthesis in response to normal levels of dietary protein or light exercise.
- Beers Criteria: A clinical guideline listing potentially inappropriate medications that should be avoided or modified in older adults.
- Conserved Transcriptional Response to Adversity (CTRA): A genomic footprint characterized by the upregulation of pro-inflammatory genes and downregulation of antiviral genes in response to chronic psychological stress or loneliness.
- Glymphatic System: The central nervous system's waste clearance pathway, which clears toxic protein aggregates (such as amyloid-beta) during slow-wave sleep.
- GrimAge: An advanced epigenetic clock that utilizes DNA methylation markers to highly predict biological aging speed and mortality risk.
- Osteosarcopenia: The concurrent presence of osteopenia/osteoporosis (bone density loss) and sarcopenia (muscle mass and function loss).
- Perturbation-Based Balance Training (PBBT): A dynamic balance conditioning program that exposes individuals to unpredictable physical displacements to train reactive motor recovery.
- Rate of Force Development (RFD): The speed at which a muscle can exert force; the key metric responsible for preventing falls during a slip.
- Sensory Reweighting: The central nervous system's capacity to dynamically prioritize stable sensory inputs (visual, vestibular, proprioceptive) based on environmental demands.
- Slow-Wave Activity (SWA): Low-frequency electroencephalographic oscillations characteristic of deep, restorative N3 sleep, critical for memory consolidation and cellular repair.
¶ 12. Methods & Search Strategy
¶ Review & Search Methodology
This guide was synthesized from a multi-disciplinary literature extraction prioritizing Tier 1 and Tier 2 human evidence. Search parameters isolated systematic reviews, meta-analyses, and randomized controlled trials (RCTs) from databases including PubMed, ClinicalTrials.gov, and the Cochrane Database of Systematic Reviews.
- Inclusion Criteria: Human subjects aged $\ge$60 years; prospective randomized designs; standardized physiological and functional endpoints (e.g., bone mineral density, Rate of Force Development, center-of-pressure sway, sleep architecture, leukocyte transcriptomics, epigenetic clock dynamics).
- Exclusion Criteria: Pre-clinical animal or in-vitro models; uncontrolled observational reports; non-peer-reviewed whitepapers.
- Evidence Grading: Clinical statements are graded using the GRADE framework. High certainty corresponds to multiple consistent, high-impact RCTs or gold-standard meta-analyses. Moderate certainty corresponds to single high-quality RCTs or strong prospective longitudinal cohorts with minor design limitations.
¶ 13. References
¶ 14. Update Log
- February 2026: Comprehensive guide page established. Integrated current evidence on perturbation-based balance training (PBBT), clinical GHRH interventions, and the definitive Phase 2b clinical trial outcomes for Laromestrocel (Lomecel-B) in aging frailty. Added 4 Nano Banana Pro Nature-like biomedical diagrams.
Hernandez-Martinez J, Branco BHM, Vasquez-Carrasco E, et al. Effects of Strength Training on Body Composition, Physical Performance, and Protein or Calcium Intake in Older People with Osteosarcopenia: A Meta-Analysis. Nutrients. 2025;17(17):3204. https://pubmed.ncbi.nlm.nih.gov/40944241/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Tøien T, Berg OK, Modena R, et al. Heavy Strength Training in Older Adults: Implications for Health, Disease and Physical Performance. Journal of Cachexia, Sarcopenia and Muscle. 2025;16(2):13645. https://pubmed.ncbi.nlm.nih.gov/40241440/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Sharma S, Szabo IZ, Danielsen MB, et al. Perturbation-Based Balance Training Reduces Falls and Fall Injuries in Older People: Insights on Mechanisms and Training Parameters From a Systematic Review. Journal of the American Medical Directors Association. 2026;27(1):106316. https://pubmed.ncbi.nlm.nih.gov/42391766/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Guo C, Yin L, Chen P. Effects of Multisensory Integration Training on Postural Stability Characteristics and Fall Risk in Older Adults: Systematic Review and Meta-Analysis. JMIR Aging. 2026;9:e27884. https://pubmed.ncbi.nlm.nih.gov/42096607/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Bauer J, Biolo G, Cederholm T, et al. Evidence-based recommendations for optimal dietary protein intake in older people: a position paper from the PROT-AGE Study Group. Journal of the American Medical Directors Association. 2013;14(8):542-559. https://pubmed.ncbi.nlm.nih.gov/23867520/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Farsijani S, Payette H, Morais JA, et al. Even mealtime distribution of protein intake is associated with greater muscle strength, but not with 3-y physical function decline, in free-living older adults: the Quebec longitudinal study on Nutrition as a Determinant of Successful Aging (NuAge study). The American Journal of Clinical Nutrition. 2017;106(1):113-124. https://pubmed.ncbi.nlm.nih.gov/28515070/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Ahmadi M, Krause AJ, O'Hora KP, et al. The association between slow wave activity and memory improvement following cognitive-behavioral therapy for insomnia in older adults: A secondary analysis of a randomized clinical trial. Journal of Clinical Sleep Medicine. 2026;22(2):11244. https://pubmed.ncbi.nlm.nih.gov/42303834/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Lemoine P, Nir T, Laudon M, et al. Prolonged-release melatonin improves sleep quality and morning alertness in insomnia patients aged 55 years and older and has no withdrawal effects. Journal of Sleep Research. 2007;16(4):372-380. https://pubmed.ncbi.nlm.nih.gov/18036082/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Ghadimi S, Erickson AJ, Vaughan M, et al. Sleep aid usage following benzodiazepine receptor agonist tapering and cognitive behavioral therapy for insomnia in middle-aged and older adults. Journal of Clinical Sleep Medicine. 2026;22(1):11182. https://pubmed.ncbi.nlm.nih.gov/42168527/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Yu L, Li B, Li N, et al. Spermidine for cognitive ageing: insights into observational and interventional studies. General Psychiatry. 2025;38(1):e101428. https://pubmed.ncbi.nlm.nih.gov/41098596/ ↩︎ ↩︎ ↩︎ ↩︎
Baker LD, Barsness SM, Borson S, et al. Effects of growth hormone–releasing hormone on cognitive function in adults with mild cognitive impairment and healthy older adults: results of a controlled trial. Archives of Neurology. 2012;69(11):1420-1428. https://pubmed.ncbi.nlm.nih.gov/22869065/ ↩︎ ↩︎ ↩︎ ↩︎
Kolykhalov IV, Androsova LV, Gavrilova SI. Clinical and immunological effects of choline alfoscerate in the treatment of amnestic type Mild Cognitive Impairment. Zhurnal nevrologii i psikhiatrii imeni S.S. Korsakova. 2022;122(11):111-118. https://pubmed.ncbi.nlm.nih.gov/36412158/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Luan T, Wang Y, Li B, et al. The effectiveness of cognitive behavioral therapy on loneliness among older adults: A systematic review and meta-analysis. Archives of Gerontology and Geriatrics. 2026;130:105642. https://pubmed.ncbi.nlm.nih.gov/41101098/ ↩︎ ↩︎ ↩︎ ↩︎
Kim ES, Nakamura JS, Strecher VJ, et al. Reduced Epigenetic Age in Older Adults With High Sense of Purpose in Life. The Journals of Gerontology. Series A, Biological Sciences and Medical Sciences. 2023;78(6):glad088. https://pubmed.ncbi.nlm.nih.gov/36966357/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Cole SW, Levine ME, Arevalo JM, et al. Loneliness, eudaimonia, and the human conserved transcriptional response to adversity. Psychoneuroendocrinology. 2015;62:11-17. https://pubmed.ncbi.nlm.nih.gov/26246388/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Seppala LJ, Wermelink AMAT, de Vries M, et al. Fall-Risk-Increasing Drugs: A Systematic Review and Meta-Analysis: II. Psychotropics. Journal of the American Medical Directors Association. 2018;19(4):337-345. https://pubmed.ncbi.nlm.nih.gov/29402652/ ↩︎ ↩︎ ↩︎ ↩︎
Sheikh-Taha M. Prevalence and predictors of potentially inappropriate medication use among older adults with heart failure: a 2023 Beers Criteria-based evaluation. BMC Geriatrics. 2026;26(1):08191. https://pubmed.ncbi.nlm.nih.gov/42277692/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Ruiz JG, Oliva AA Jr, Ramdas KN, et al. Randomized phase 2b dose-escalation trial of stem cell therapy with laromestrocel for aging frailty. Cell Stem Cell. 2026;33(2):1016. https://pubmed.ncbi.nlm.nih.gov/41747733/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Lee BC, Kim KI, Lee J, et al. Effects of resistance training on osteosarcopenia in community-dwelling postmenopausal Korean women: Randomised controlled ERTO-K trial. Experimental Gerontology. 2025;198:112450. https://pubmed.ncbi.nlm.nih.gov/40825414/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Hoodless S, Ventre J, Smith SK, et al. Implementation of Falls Management Exercise (FaME) falls prevention programme among community-dwelling older adults. A scoping review. BMC Public Health. 2026;26(1):19342. https://pubmed.ncbi.nlm.nih.gov/42288799/ ↩︎ ↩︎ ↩︎ ↩︎
Wang Y, Wang Y, Wang F, et al. Combined vitamin K(2) and D(3) therapy improves endoscopic fusion outcomes in osteoporotic lumbar degenerative disease: a prospective study. Scientific Reports. 2025;15(1):95021. https://pubmed.ncbi.nlm.nih.gov/40316739/ ↩︎ ↩︎
Alghosi M, Khazanin H, Faraji S. The effect of FallProof exercise programs on balance, fear of falling and quality of life in older adults: a systematic review with meta-analysis. BMC Geriatrics. 2026;26(1):08541. https://pubmed.ncbi.nlm.nih.gov/41776466/ ↩︎ ↩︎ ↩︎ ↩︎
Silveira EA, Souza GVE, Rodrigues LP, et al. Effectiveness of physical exercise on osteosarcopenia in older adults: A systematic review. Geriatric Nursing. 2026;54:1016. https://pubmed.ncbi.nlm.nih.gov/41637773/ ↩︎ ↩︎
Schwarz C, Benson GS, Horn N, et al. Effects of Spermidine Supplementation on Cognition and Biomarkers in Older Adults With Subjective Cognitive Decline: A Randomized Clinical Trial. JAMA Network Open. 2022;5(5):e2213811. https://pubmed.ncbi.nlm.nih.gov/35616942/ ↩︎ ↩︎