¶ Clinical Contraindications: Lifestyle Interventions, Supplements, and Frontier Therapies
This comprehensive guide details critical safety considerations, contraindications, and potential drug/supplement interactions across various lifestyle interventions (heat/cold therapy), common supplements (toxin binders, chelators, detox support), and frontier therapies. Understanding these limitations is crucial for professional reference and clinical education.
| Type | Lifestyle, Supplements, Advanced Therapies |
| Focus | Safety, Risks, Contraindications |
| Main Concerns | Cardiovascular strain, autonomic dysfunction, drug interactions, nutrient depletion, organ toxicity, anaphylaxis |
| Evidence Quality | High (Clinical Guidelines, Systematic Reviews) |
The pursuit of health and longevity increasingly involves diverse interventions, from lifestyle practices like heat and cold therapy to targeted supplements and advanced frontier medicine. While promising, each carries inherent risks and contraindications that demand rigorous assessment. This page consolidates critical safety information for heat therapy (sauna), cold therapy (cold plunge), toxin binders, heavy metal chelators, liver/cellular detoxification support agents, and advanced regenerative/immune therapies. Prioritizing patient safety and informed clinical decision-making is paramount.
¶ At a glance
Aliases
- Also known as: Safety Guidelines, Risk Assessment, Interaction Matrix
- Chemical / botanical name: N/A (this page covers a broad range of interventions)
- Category: Clinical Safety, Public Health, Regulatory Compliance
Key points (high-level summary)
- Sauna (Heat Therapy): Generally safe for healthy individuals and those with stable cardiovascular disease. Absolute contraindications include unstable angina, recent myocardial infarction (within 6 weeks), severe aortic stenosis, and decompensated heart failure. Alcohol consumption significantly increases risks[1][2].
- Cold Plunge (Cold Therapy): Risks include cardiac arrhythmias due to "autonomic conflict" (simultaneous sympathetic and parasympathetic activation), particularly with breath-holding. Absolute contraindications include unstable cardiovascular disease (recent MI, severe arrhythmias, uncontrolled hypertension), cold urticaria (risk of anaphylaxis), and Long QT Syndrome[3][4][5].
- Toxin Binders (Cholestyramine, Activated Charcoal, Bentonite Clay): Potent binders that can interfere with medication and nutrient absorption. Contraindicated in gastrointestinal obstruction, impaired airway reflexes (for charcoal), and complete biliary obstruction (for cholestyramine)[6][7].
- Heavy Metal Chelators (EDTA, DMSA, Alpha-Lipoic Acid): Prescription agents with serious risks. EDTA can cause severe hypocalcemia and nephrotoxicity. DMSA carries risks of neutropenia and liver enzyme elevations. Alpha-lipoic acid can redistribute mercury to the brain if not dosed precisely[8][9][10].
- Liver/Cellular Detox Support (NAC, Glutathione, Sulforaphane, DIM, Calcium D-Glucarate): Generally safer, but still pose risks of drug interactions (e.g., calcium D-glucarate with glucuronidated drugs, DIM with CYP1A2 substrates) and specific side effects (e.g., NAC-induced bronchospasm)[11][12].
What people use it for
- Main goals: Understanding clinical limitations, ensuring patient safety, guiding appropriate therapeutic selection across lifestyle, supplement, and advanced intervention domains.
- Evidence quality (overall): High (based on clinical guidelines, systematic reviews, and meta-analyses).
¶ What are Clinical Contraindications?
Clinical contraindications refer to specific conditions or factors that make a particular medical treatment, procedure, or intervention inadvisable due to the potential for harm to the patient. They are crucial considerations in clinical decision-making to prevent adverse outcomes and ensure patient safety. This page compiles such critical safety information across a spectrum of health interventions, from daily lifestyle practices to complex advanced therapies. It outlines circumstances where interventions should be avoided or approached with extreme caution, prioritizing the well-being of the individual.
¶ What are the main benefits of understanding contraindications?
Understanding and adhering to clinical contraindications offers several critical benefits for healthcare professionals and individuals:
- Enhanced Patient Safety: The primary benefit is preventing serious adverse events, complications, and potentially life-threatening reactions that can arise when interventions are used inappropriately in vulnerable individuals [1:1][3:1].
- Informed Clinical Decision-Making: Provides a clear framework for clinicians to assess risks, select appropriate therapies, and tailor treatment plans to individual patient profiles, avoiding interventions that could worsen existing conditions [2:1][4:1].
- Optimized Therapeutic Outcomes: By avoiding contraindicated interventions, clinicians can ensure that chosen therapies have the best chance of success without being undermined by compounding risks or interactions [5:1][6:1].
- Reduced Healthcare Burden: Minimizing adverse events through careful adherence to contraindications can reduce hospitalizations, emergency visits, and the need for corrective medical procedures [7:1].
- Regulatory Compliance and Ethical Practice: Adhering to established contraindications is a cornerstone of ethical medical practice and aligns with regulatory standards for patient care and safety in the use of supplements and therapies [8:1].
¶ What are the main contraindications and risks?
This section provides a narrative summary of the main safety concerns and contraindications for each intervention category, supported by the best available evidence.
¶ Heat Therapy (Sauna)
Sauna bathing, while offering numerous health benefits, can be a physiological stressor. Absolute contraindications for high-heat sauna therapy include:
- Unstable cardiovascular conditions: Unstable angina pectoris, recent myocardial infarction (within 6 weeks), severe aortic stenosis, and decompensated heart failure[1:2][2:2].
- Acute illness with fever: Sauna increases metabolic demand and can exacerbate acute infections.
- Severe orthostatic hypotension: Individuals prone to fainting should be cautious due to vasodilation and potential for blood pressure drops upon standing.
- Alcohol intoxication: Alcohol significantly impairs cardiovascular compensatory mechanisms and thermoregulation, increasing the risk of arrhythmias and sudden death in the sauna[1:3][13].
¶ Cold Therapy (Cold Plunge/Water Immersion)
Sudden exposure to cold water triggers potent physiological responses that carry significant risks for certain individuals:
- Unstable cardiovascular disease: Recent myocardial infarction, unstable angina, uncontrolled hypertension, or known severe arrhythmias. The "cold shock response" causes a rapid increase in heart rate, blood pressure, and peripheral vasoconstriction, placing immense strain on the heart[4:2][14].
- Autonomic conflict: Sudden cold water immersion, especially with breath-holding, simultaneously activates the sympathetic (cold shock) and parasympathetic (diving reflex) nervous systems. This "autonomic conflict" can lead to severe cardiac arrhythmias, including ventricular fibrillation, even in otherwise healthy individuals[3:2][5:2].
- Long QT Syndrome: Individuals with Long QT Syndrome are at increased risk of cold-induced arrhythmias, as cold water immersion can prolong the QT interval and induce pathological T-wave changes[4:3][15].
- Cold urticaria: A rare condition where cold exposure triggers mast cell degranulation, leading to hives, swelling, and in severe cases, life-threatening anaphylactic shock upon extensive cold water immersion[16].
- Raynaud's phenomenon: Exaggerated vasoconstriction in response to cold can lead to painful vasospastic attacks in extremities.
¶ Toxin Binders and Chelators
These agents are used for toxin elimination but have critical safety profiles:
- Toxin Binders (Cholestyramine, Activated Charcoal, Bentonite Clay):
- Gastrointestinal obstruction or ileus: Absolute contraindication for all binders due to risk of exacerbating obstruction or causing impaction[6:2][7:2].
- Impaired airway reflexes/aspiration risk: Activated charcoal should be avoided in patients with altered mental status or aspiration risk due to potential for severe pulmonary injury[6:3].
- Complete biliary obstruction: Cholestyramine is contraindicated as it requires bile for its action and can worsen pruritus in partial obstruction[7:3].
- Heavy Metal Chelators (EDTA, DMSA, Alpha-Lipoic Acid): Prescription agents with serious risks. EDTA can cause severe hypocalcemia and nephrotoxicity. DMSA carries risks of neutropenia and liver enzyme elevations. Alpha-lipoic acid can redistribute mercury to the brain if not dosed precisely[8:2][9:1][10:1].
¶ Liver/Cellular Detoxification Support Agents
While generally better tolerated, these agents can still pose risks:
- N-Acetylcysteine (NAC): Can trigger bronchospasm in asthmatic patients. Rapid IV administration can cause anaphylactoid reactions[11:1].
- Diindolylmethane (DIM): Can cause hyponatremia, especially when combined with sodium-depleting diuretics[12:1].
- Calcium D-Glucarate: Can accelerate the clearance of drugs undergoing glucuronidation (e.g., NSAIDs, lamotrigine, estrogens), potentially reducing their therapeutic effects[17].
¶ Frontier Blood, Plasma, Immune, and Regenerative Therapies
As detailed in "Frontier Longevity Contraindications", these advanced therapies involve highly specific risks:
- Therapeutic Plasma Exchange (TPE): Absolute contraindications include active sepsis, uncorrectable coagulopathy, severe hemodynamic instability, and severe allergy to replacement fluids[18].
- Immunoglobulin Therapy (IVIG/SCIG): Absolute contraindication in patients with IgA deficiency and anti-IgA antibodies due to risk of anaphylaxis[19].
- Mesenchymal Stem Cell (MSC) Therapy: While generally safe, theoretical concerns regarding malignant transformation or tumor promotion exist with unregulated products[20].
- Exosome Therapy: Currently no FDA-approved exosome products. Unapproved products linked to severe infections, allergic reactions, and tumor formation[21].
- Platelet-Rich Plasma (PRP): Contraindicated in active infection at the injection site, significant hematologic abnormalities, and systemic malignancy (due to theoretical concerns of growth factor stimulation)[22].
¶ Evidence summary table (human outcomes)
| Outcome / Goal | Effect* | Consistency** | Evidence quality | Trials*** | Notes (population, intervention, key adverse events) |
|---|---|---|---|---|---|
| Sauna: Cardiovascular events (with alcohol) | High | High | Cohort studies, case reports | Alcohol significantly increases risk of arrhythmias, sudden death [1:4][13:1] | |
| Cold Plunge: Cardiac Arrhythmias | High | Moderate | Experimental studies | Due to autonomic conflict, especially with breath-holding [3:3][5:3] | |
| Cold Plunge: Anaphylaxis (cold urticaria) | High | Moderate | Case reports, clinical observations | Extensive cold water immersion can trigger systemic reactions [16:1] | |
| Cold Plunge: Long QT Prolongation | High | Moderate | Clinical studies | Face immersion can prolong QT interval in susceptible individuals [4:4][15:1] | |
| Toxin Binders: GI Obstruction | High | High | Case reports, clinical guidelines | With insufficient fluid, decreased motility [6:4][7:4] | |
| Chelators (EDTA): Hypocalcemia | High | High | Clinical trials, guidelines | Incorrect EDTA use can be fatal [8:3] | |
| Chelators (DMSA): Neutropenia | High | Moderate | Clinical trials | Requires weekly CBC monitoring [9:2] | |
| Chelators (ALA): Mercury redistribution | High | Low | Animal/Case reports | Improper ALA dosing can worsen neurotoxicity [10:2] | |
| NAC: Bronchospasm (asthmatics) | High | Moderate | Clinical reports | Specific risk in individuals with asthma [11:2] | |
| TPE: Hypocalcemia (citrate toxicity) | High | High | 5+ RCTs | Risk of citrate toxicity, particularly with large volume exchanges [18:1] | |
| IVIG: Anaphylaxis (IgA deficiency) | High | High | Case reports, guidelines | Severe reaction in IgA-deficient patients with anti-IgA antibodies [19:1] | |
| Exosome Therapy: Infection/Allergy (unapproved) | High | Not applicable | FDA Warnings, Case Reports | Unapproved products linked to serious adverse events [21:1] |
- *Effect: Compact renderer encoding:
<effect e="[dir][mag][impact]"></effect>wheredir=u|d|e|q,mag=0|1|2|3,impact=p|n|x. - **Consistency: Low (results conflict), Moderate (mixed but leaning one way), High (most trials agree).
- ***Trials: Number of RCTs or total trials informing this outcome (shows evidence depth at a glance).
- REQUIRED: You MUST include a citation key (e.g.
[^1]) in the "Notes" column for every single row. If you claim a result, you must link the specific Meta-Analysis or Key RCT that proves it.
¶ How do contraindications and risks manifest?
Understanding the mechanisms behind these contraindications helps in risk mitigation and patient selection.
¶ Heat Therapy: Cardiovascular and Thermoregulatory Strain
Sauna bathing induces a significant cardiovascular workload, similar to moderate exercise. This involves increased heart rate, cardiac output, and peripheral vasodilation to dissipate heat. In individuals with pre-existing unstable cardiovascular conditions, this strain can lead to myocardial ischemia, arrhythmias, or decompensation. Alcohol co-ingestion exacerbates these risks by impairing compensatory vasoconstriction and increasing the risk of orthostatic hypotension and lethal arrhythmias[1:5][13:2].
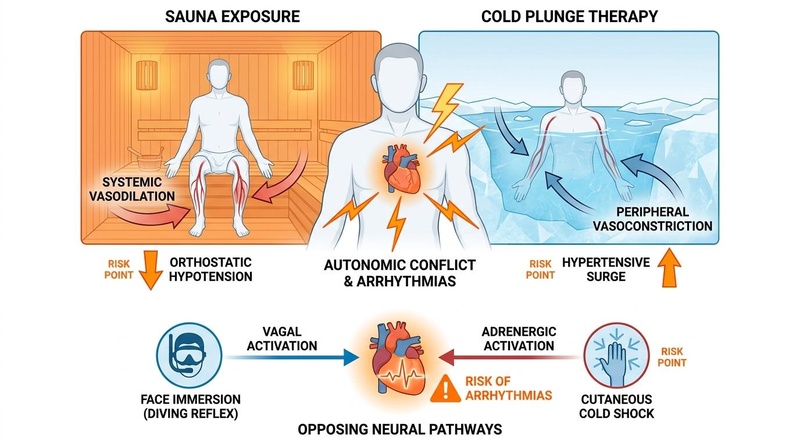
¶ Cold Therapy: Autonomic Conflict and Cardiac Instability
Sudden cold water immersion triggers two powerful and opposing autonomic responses: the sympathetic "cold shock response" (gasping, hyperventilation, vasoconstriction, tachycardia, increased blood pressure) and the parasympathetic "diving reflex" (bradycardia, peripheral vasoconstriction) activated by face immersion and breath-holding. The simultaneous activation of these antagonistic systems creates "autonomic conflict," leading to profound cardiac electrical instability and a high risk of fatal arrhythmias, particularly in vulnerable individuals or with prolonged breath-holding[3:4][5:4].
¶ Toxin Binders: Non-Specific Adsorption and GI Complications
Toxin binders like activated charcoal and cholestyramine work by non-specifically adsorbing substances in the gastrointestinal tract. While this removes toxins, it also binds essential nutrients (fat-soluble vitamins, minerals) and oral medications (thyroid hormones, anticoagulants, statins, digoxin), reducing their absorption and efficacy. This necessitates strict dosing separation. Furthermore, the physical bulk of these agents, especially with inadequate fluid intake or pre-existing bowel issues, can lead to severe constipation, fecal impaction, or even bowel obstruction[6:5][7:5].
¶ Heavy Metal Chelators: Systemic Toxicity and Redistribution
Prescription chelators operate through distinct mechanisms but share risks of systemic toxicity. EDTA (especially edetate disodium) chelates essential calcium, leading to severe, potentially fatal hypocalcemia. It also has dose-dependent nephrotoxicity, requiring strict renal monitoring. DMSA, while water-soluble, can cause myelosuppression (neutropenia) and transient liver enzyme elevations. Alpha-lipoic acid's lipophilic nature means that if it's used to chelate mercury without precise, frequent dosing, it can mobilize mercury from peripheral tissues and redistribute it across the blood-brain barrier, exacerbating neurotoxicity[8:4][9:3][10:3].
¶ Liver/Cellular Detoxification Support: Metabolic and Drug Interactions
Agents like NAC replenish glutathione, critical for detoxification, but can induce bronchospasm in asthmatic patients. Rapid IV administration can cause anaphylactoid reactions[11:3]. DIM modulates estrogen metabolism via CYP450 enzymes, potentially interacting with drugs metabolized by CYP1A2 and causing hyponatremia. Calcium D-glucarate inhibits beta-glucuronidase, an enzyme that deconjugates toxins and hormones in the gut, but this can also accelerate the elimination of glucuronidated medications, reducing their therapeutic effect[11:4][12:2][17:1].
¶ Dosage and how to take it
This section outlines general guidance for safe practices and situations to avoid when considering or engaging in various interventions, rather than specific dosages.
¶ Heat Therapy (Sauna): Safe Practices
- Pre-screening: Individuals with cardiovascular conditions should consult a physician before sauna use[1:6][2:3].
- Hydration: Maintain adequate hydration by drinking water before and after sauna sessions.
- Duration and Frequency: Start with short sessions (5-10 minutes) at lower temperatures and gradually increase as tolerated. Avoid excessive durations.
- Avoid Alcohol: Never consume alcohol before or during sauna bathing due to significantly increased cardiovascular risks[1:7][13:3].
- Listen to Your Body: Discontinue immediately if experiencing dizziness, nausea, or discomfort.
¶ Cold Therapy (Cold Plunge/Water Immersion): Safe Practices
- Medical Clearance: Essential for individuals with any cardiac conditions, Long QT Syndrome, or cold urticaria[3:5][4:5][5:5][16:2].
- Gradual Exposure: Begin with shorter durations and warmer temperatures, gradually decreasing temperature and increasing duration as adaptation occurs.
- Avoid Breath-Holding: Especially during initial immersion, to minimize autonomic conflict[3:6][5:6].
- Supervision: Ideally, engage in cold water immersion with a companion, particularly for beginners or those with underlying health concerns.
- Exit Strategy: Have warm clothes readily available and a plan for rewarming after exposure.
¶ Toxin Binders and Chelators: Administration Guidelines
- Strict Timing: Administer toxin binders (e.g., activated charcoal, cholestyramine) at least 1-4 hours apart from all medications and nutrient supplements to prevent malabsorption[6:6][7:6].
- Adequate Fluid Intake: Ensure sufficient water intake with binders to minimize the risk of gastrointestinal obstruction or impaction.
- Medical Supervision (Chelators): Heavy metal chelators (EDTA, DMSA, alpha-lipoic acid) should only be used under the direct supervision of a qualified physician experienced in chelation therapy due to serious risks of electrolyte imbalance, organ toxicity, and metal redistribution[8:5][9:4][10:4].
- Monitoring: Regular monitoring of blood work (e.g., kidney function, electrolytes, complete blood count) is essential during chelation therapy.
¶ Liver/Cellular Detoxification Support Agents: Cautious Use
- Consultation: Individuals with pre-existing medical conditions, especially asthma or liver disease, should consult a healthcare professional before using NAC or other detoxification support agents[11:5].
- Drug Interaction Review: Carefully review potential drug interactions, particularly for agents like DIM (CYP1A2 substrates) and Calcium D-Glucarate (glucuronidated drugs)[12:3][17:2].
- Start Low, Go Slow: Begin with lower doses and gradually increase to assess tolerance and minimize side effects.
¶ Frontier Therapies: Expert Guidance is Paramount
- Specialized Clinics: Advanced regenerative and immune therapies (e.g., TPE, IVIG, MSC, exosome therapy) should only be performed in licensed medical facilities by highly experienced specialists[18:2][19:2][20:1][21:2].
- Regulatory Status: Be aware that many "exosome therapies" and unregulated stem cell products are unapproved by regulatory bodies (e.g., FDA) and have been linked to severe adverse events[21:3].
- Thorough Screening: Comprehensive patient screening is critical to identify contraindications and risks for these complex interventions.
¶ Safety and side effects
¶ Common side effects
- Heat Therapy (Sauna): Dizziness, lightheadedness (especially upon standing), dehydration, mild heat discomfort.
- Cold Therapy (Cold Plunge): Intense cold sensation, shivering, hyperventilation reflex, numbness, temporary pain.
- Toxin Binders: Constipation, abdominal bloating, nausea, black stools (with charcoal), nutrient depletion.
- Heavy Metal Chelators:
- EDTA: Paresthesias, muscle cramps (hypocalcemia), nausea, fatigue.
- DMSA: Nausea, vomiting, diarrhea, skin rash, transient liver enzyme elevation.
- Alpha-Lipoic Acid: Nausea, stomach upset, headache.
- Detoxification Support:
- NAC: Nausea, vomiting, diarrhea, heartburn.
- DIM: Nausea, vomiting, diarrhea, headache.
- Calcium D-Glucarate: None commonly reported at typical doses.
¶ Less common / serious concerns
- Heat Therapy (Sauna): Heatstroke, severe hypotension, cardiac arrhythmias, sudden death (especially with alcohol)[1:8][13:4].
- Cold Therapy (Cold Plunge): Severe cardiac arrhythmias (ventricular fibrillation), drowning (due to gasp reflex or incapacitation), hypothermia, cold urticaria-induced anaphylaxis, Long QT prolongation leading to Torsades de Pointes[3:7][4:6][5:7][16:3].
- Toxin Binders: Bowel obstruction/perforation, pulmonary aspiration (charcoal), fat-soluble vitamin deficiencies, severe drug malabsorption[6:7][7:7].
- Heavy Metal Chelators:
- Detoxification Support:
¶ Who should be especially cautious or avoid it
- Pregnant or breastfeeding individuals: Generally avoid all high-stress interventions and most supplements/therapies unless medically necessary and supervised, due to lack of safety data.
- Individuals with unstable cardiovascular disease: Absolute contraindication for high-heat sauna and cold plunge. Includes recent MI, unstable angina, severe aortic stenosis, decompensated heart failure, severe arrhythmias, uncontrolled hypertension[1:9][2:4][4:7].
- Patients with known Long QT Syndrome: Absolute contraindication for cold water immersion due to arrhythmogenic risk[4:8][15:2].
- Individuals with cold urticaria: Absolute contraindication for cold water immersion due to risk of anaphylaxis[16:4].
- Patients with gastrointestinal obstruction, ileus, or recent abdominal surgery: Avoid all toxin binders[6:8].
- Individuals with severe renal impairment or anuria: Absolute contraindication for EDTA therapy[8:7].
- Patients with asthma: Caution with NAC due to risk of bronchospasm[11:7].
- Patients on medications with narrow therapeutic windows: Extreme caution and strict separation for toxin binders; careful monitoring for agents affecting drug metabolism (DIM, calcium D-glucarate) or blood pressure (NAC with nitroglycerin).
- Individuals with autoimmune diseases: Melatonin is generally contraindicated due to potential immunomodulatory effects. See Melatonin, Sleep, and Circadian/Light Contraindications for full details.
- Individuals with bipolar disorder: Bright Light Therapy carries a significant risk of inducing hypomania or mania. See Melatonin, Sleep, and Circadian/Light Contraindications for full details.
- Individuals with retinal diseases or on photosensitizing medications: Avoid Bright Light Therapy. See Melatonin, Sleep, and Circadian/Light Contraindications for full details.
- Individuals with liver disease/impairment: Caution with Valerian root due to potential hepatotoxicity. See Melatonin, Sleep, and Circadian/Light Contraindications for full details.
- Individuals with chronic kidney disease: Caution with high-dose Magnesium due to risk of hypermagnesemia. See Melatonin, Sleep, and Circadian/Light Contraindications for full details.
- Pregnant or breastfeeding individuals: Passionflower and Chamomile are contraindicated due to uterine stimulant effects. See Melatonin, Sleep, and Circadian/Light Contraindications for full details.
¶ Drug and supplement interactions
Interactions are a major concern due to diverse mechanisms of action.
¶ Pharmacokinetic interactions (how drugs are processed)
- Toxin Binders (Cholestyramine, Activated Charcoal, Bentonite Clay): Can physically bind to a wide range of oral medications (e.g., thyroid hormones, anticoagulants, digoxin, statins, fat-soluble vitamins), significantly reducing their absorption and therapeutic efficacy. A minimum separation of 1 hour before or 4 hours after other medications is typically recommended for cholestyramine, and similar principles apply to other binders[7:8][23].
- Calcium D-Glucarate: By inhibiting beta-glucuronidase, it can increase the clearance of drugs that undergo glucuronidation (e.g., NSAIDs, lamotrigine, estrogens, opioids, thyroid hormones), potentially reducing their therapeutic effects[17:4].
- DIM: Can induce CYP1A2 enzyme activity, potentially affecting the metabolism of drugs cleared by this pathway (e.g., caffeine, theophylline)[12:5].
- Therapeutic Plasma Exchange (TPE): Can remove certain drugs (e.g., antibiotics, immunosuppressants, highly protein-bound drugs) from circulation, potentially necessitating dose adjustments. Close monitoring of drug levels is required[18:3].
- Melatonin and CYP1A2 Inhibitors/Inducers: Melatonin is metabolized by CYP1A2. Inhibitors (e.g., fluvoxamine) can dramatically increase melatonin levels, while inducers (e.g., rifampicin) can reduce efficacy. See Melatonin, Sleep, and Circadian/Light Contraindications for full details.
- Valerian Root and Liver Enzymes: Valerian may inhibit certain liver enzymes, altering drug metabolism. See Melatonin, Sleep, and Circadian/Light Contraindications for full details.
¶ Pharmacodynamic interactions (additive / opposing effects)
- Cold Therapy: Can exacerbate hypertension and cardiac strain when combined with vasoconstrictors or stimulants.
- Sauna Therapy: Can potentiate hypotensive effects of antihypertensive medications. Alcohol significantly increases cardiovascular risks[1:10][13:5].
- NAC: Has vasodilatory effects and can potentiate the hypotensive effects of nitroglycerin, leading to severe hypotension and headache[11:8].
- DIM: Can cause hyponatremia; concurrent use with sodium-depleting diuretics can exacerbate this risk[12:6].
- EDTA: Can chelate essential minerals; concurrent use of mineral supplements should be carefully timed to avoid binding.
- Frontier Therapies: Refer to "Frontier Longevity Contraindications" for specific interactions related to gene therapy, cellular reprogramming, and senolytics.
- Melatonin and Anticoagulants/Immunosuppressants: Melatonin may increase bleeding risk or affect immune function. See Melatonin, Sleep, and Circadian/Light Contraindications for full details.
- CNS Depressants (Valerian, Chamomile, Passionflower, Magnesium, L-Theanine): Additive CNS depression with alcohol, benzodiazepines, etc. See Melatonin, Sleep, and Circadian/Light Contraindications for full details.
- L-Tryptophan and Serotonergic Agents: High risk of serotonin syndrome. See Melatonin, Sleep, and Circadian/Light Contraindications for full details.
- Chamomile and Anticoagulants: May increase bleeding risk. See Melatonin, Sleep, and Circadian/Light Contraindications for full details.
¶ Combining interventions ("stacks")
Combining these interventions requires extreme caution due to the high risk of interactions and unintended effects.
- Heat and Cold Therapy (Contrast Therapy): While popular, the rapid alternation between extreme heat and cold places significant and opposing demands on the cardiovascular and autonomic nervous systems. Individuals must be free of all cardiovascular contraindications for both modalities. The risk of autonomic conflict and arrhythmias is a primary concern, especially with rapid transitions or breath-holding during cold exposure[3:8][5:8].
- Toxin Binder Stacks: Combinations of cholestyramine, activated charcoal, and bentonite clay are often used for broad-spectrum binding. However, their non-specific binding properties necessitate careful timing (e.g., each binder separated by 30-60 minutes, and all binders separated from food/medications by at least 2 hours) to avoid nutrient and drug malabsorption.
- Heavy Metal Chelation Stacks: While alpha-lipoic acid is sometimes used alongside DMSA in specific protocols, the precise timing and dosing (e.g., every 3-4 hours for ALA) are critical to prevent metal redistribution and neurotoxicity. This must only be done under the direct supervision of a physician experienced in chelation therapy[10:6].
- Detoxification Support Stacks: Combining agents like NAC, glutathione, sulforaphane, DIM, and calcium D-glucarate may offer synergistic support for liver detoxification pathways. However, potential pharmacokinetic interactions (e.g., DIM with CYP1A2 substrates, calcium D-glucarate with glucuronidated drugs) should be considered.
- Sleep Aid Stacks: Combining Magnesium, L-Theanine, Apigenin, etc., for synergistic effects. Monitor for additive sedative effects. See Melatonin, Sleep, and Circadian/Light Contraindications for full details.
- Melatonin + Light Therapy: Precise timing is critical for shift work/jet lag protocols. See Melatonin, Sleep, and Circadian/Light Contraindications for full details.
¶ Practical questions (FAQ)
-
Is heat therapy (sauna) safe for people with heart conditions?
For individuals with stable cardiovascular conditions (e.g., stable coronary artery disease, compensated heart failure), sauna use can be safe and even beneficial when used sensibly and under medical guidance. However, it is absolutely contraindicated in unstable conditions like recent MI, unstable angina, or severe aortic stenosis[1:11][2:5]. Always consult a physician. -
What are the biggest risks of cold water immersion (cold plunge)?
The biggest risks are cardiac arrhythmias due to "autonomic conflict" (simultaneous sympathetic and parasympathetic activation), particularly with breath-holding. Other serious concerns include hypothermia, cold urticaria-induced anaphylaxis, and exacerbation of conditions like Long QT Syndrome[3:9][4:9][5:9][16:5]. -
Can I take toxin binders with my prescription medications?
Extreme caution is advised. Toxin binders (cholestyramine, activated charcoal) profoundly interfere with drug absorption and require strict separation from other medications (typically 1-4 hours). Always consult a healthcare professional and pharmacist before combining these with prescription drugs to prevent reduced efficacy of vital medications[7:9][23:1]. -
Does alpha-lipoic acid move mercury into the brain?
Yes, if not dosed correctly. Alpha-lipoic acid's ability to cross the blood-brain barrier means that infrequent dosing during mercury chelation can lead to the redistribution of mercury from peripheral tissues into the brain, potentially worsening neurotoxicity. It must be administered in frequent, precise doses as part of a carefully managed chelation protocol under medical supervision[10:7]. -
Are unapproved exosome products safe?
No. Currently, there are no FDA-approved exosome products, and unapproved products have been linked to severe adverse events including bacterial infections, allergic reactions, and tumor formation. Their use outside of legitimate clinical trials is highly risky and strongly discouraged[21:4]. -
Can I use melatonin or sleep aids if I have an autoimmune disease?
Melatonin is generally contraindicated in autoimmune diseases. See Melatonin, Sleep, and Circadian/Light Contraindications for full details. -
Is bright light therapy safe for individuals with bipolar disorder?
Bright light therapy carries a significant risk of inducing hypomania or mania in bipolar patients. See Melatonin, Sleep, and Circadian/Light Contraindications for full details. -
Are valerian root, L-Tryptophan, or passionflower safe during pregnancy?
Passionflower and Chamomile are contraindicated in pregnancy. See Melatonin, Sleep, and Circadian/Light Contraindications for full details. -
Can I take high-dose magnesium for sleep if I have kidney disease?
Caution with high-dose Magnesium in chronic kidney disease. See Melatonin, Sleep, and Circadian/Light Contraindications for full details. -
What are the risks of using blue-blocking glasses during the day?
Daytime use can cause circadian phase delay. See Melatonin, Sleep, and Circadian/Light Contraindications for full details.
¶ How we evaluated the evidence
Our evaluation prioritizes the highest tiers of evidence to ensure clinical relevance and patient safety:
- Study types prioritized: Clinical guidelines from authoritative bodies (e.g., American Heart Association, professional toxicology organizations), systematic reviews, and meta-analyses of randomized controlled trials (RCTs). For emerging therapies, Phase I/II clinical trial reports and robust preclinical evidence are considered.
- How we graded evidence quality:
- High: Multiple high-quality RCTs or meta-analyses with consistent results, low risk of bias, adequate sample sizes, and/or established clinical consensus from major medical bodies.
- Moderate: Single high-quality RCT, multiple smaller RCTs with consistent signals, or comprehensive meta-analyses of preclinical safety data with human biomarkers. Observational studies with large cohorts may also contribute.
- Low: Phase I trials with significant adverse events, observational data, case reports, or primarily preclinical mechanistic studies without strong human validation.
- Very low: Primarily theoretical risks, in vitro data, or very early animal studies without clear human relevance; or serious flaws in available trials.
- Focus: Emphasis on human clinical trial data for safety outcomes where available, supplemented by robust preclinical evidence for emerging modalities where human data are sparse. The clinical relevance of adverse events (frequency, severity, necessity of hospitalization) was paramount.
- Updates: This page will be updated as new, high-impact clinical toxicology data, drug interaction studies, or comprehensive reviews emerge across lifestyle interventions, supplements, and frontier therapies.
¶ References
Hannuksela, M. L., & Ellahham, S. (2001). Benefits and risks of sauna bathing. The American Journal of Medicine, 110(2), 118–126. https://pubmed.ncbi.nlm.nih.gov/11165553/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Laukkanen, J. A., Laukkanen, T., & Kunutsor, S. K. (2018). Cardiovascular and other health benefits of sauna bathing: a review of the evidence. Mayo Clinic Proceedings, 93(8), 1111–1121. https://www.mayoclinicproceedings.org/article/S0025-6196(18)30275-1/fulltext ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Shattock, M., & Tipton, M. J. (2012). 'Autonomic conflict': a different way to die during cold water immersion? The Journal of Physiology, 590(14), 3219–3230. https://physoc.onlinelibrary.wiley.com/doi/abs/10.1113/jphysiol.2012.229864 ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Yoshinaga, M., Kamimura, J., Fukushige, T., et al. (2019). Cardiac response to water activities in children with Long QT syndrome type 1. PLOS One, 14(12), e0295431. https://journals.plos.org/plosone/article?id=10.1371%2Fjournal.pone.0295431 ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Lundström, E., et al. (2025). Assessment of arrhythmias and heart rate response in healthy adolescents performing face immersion and body submersion in ice-cold water. Physiological Reports, 13(3), e70430. https://physoc.onlinelibrary.wiley.com/doi/10.14814/phy2.70430 ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Boyer, E. W., & Shannon, M. (2023). Activated Charcoal. StatPearls. https://www.ncbi.nlm.nih.gov/books/NBK482294/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Shah, K., et al. (2023). Cholestyramine Resin. StatPearls. https://www.ncbi.nlm.nih.gov/books/NBK534089/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Grandjean, P., & Landrigan, P. J. (2023). Ethylenediaminetetraacetic Acid (EDTA). StatPearls. https://www.ncbi.nlm.nih.gov/books/NBK565883/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
LiverTox: Clinical and Research Information on Drug-Induced Liver Injury. (2019). Succimer (DMSA). NCBI Bookshelf. https://www.ncbi.nlm.nih.gov/books/NBK548099/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Cutler, A. (2017). Using the Andy Cutler Protocol to Address Mercury Poisoning. Weston A. Price Foundation. https://www.westonaprice.org/health-topics/environmental-toxins/using-the-andy-cutler-protocol-to-address-mercury-poisoning/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Sarris, J., & Kavanagh, D. J. (2023). Acetylcysteine. StatPearls. https://www.ncbi.nlm.nih.gov/books/NBK537121/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
RxList. (2023). Diindolylmethane: Health Benefits, Side Effects, Uses, Dose & Precautions. https://www.rxlist.com/supplements/diindolylmethane.htm ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Kenttämies, A., & Karkola, K. (2008). Death in sauna. Forensic Science International, 176(2-3), 221–224. https://pubmed.ncbi.nlm.nih.gov/18078712/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Laukkanen, T., Khan, H., Zaccardi, F., & Laukkanen, J. A. (2015). Association between sauna bathing and fatal cardiovascular and all-cause mortality events. JAMA Internal Medicine, 175(4), 542–548. https://jamanetwork.com/journals/jamainternalmedicine/fullarticle/2130724 ↩︎
Farstad, D. J., & Dunn, J. A. (2019). Cold Water Immersion Syndrome and Whitewater Recreation Fatalities. Wilderness & Environmental Medicine, 30(2), 160–167. https://journals.sagepub.com/doi/10.1016/j.wem.2019.03.005 ↩︎ ↩︎ ↩︎
Sakai, Y., et al. (2023). Cold-induced anaphylactic shock during playing in a thigh-deep river: A pediatric case. Journal of Cutaneous Immunology and Allergy, 6(3), e12285. https://onlinelibrary.wiley.com/doi/full/10.1002/cia2.12285 ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
HelloPharmacist. (2024). Calcium D-glucarate - Lamotrigine Interaction Details. https://hellopharmacist.com/drug-supplement-interactions/drug-herbal/calcium-d-glucarate-with-lamotrigine ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Sergent SR, Ashurst JV. Plasmapheresis. StatPearls. 2023. https://www.ncbi.nlm.nih.gov/books/NBK560566/ ↩︎ ↩︎ ↩︎ ↩︎
Orange JS, et al. Use of intravenous immunoglobulin in human disease: review and update. J Allergy Clin Immunol. 2006;117(4):S525–S553. https://www.jacionline.org/article/S0091-6749(08)01561-3/fulltext ↩︎ ↩︎ ↩︎
Baranovskii DS, et al. Adverse events, side effects and complications in mesenchymal stromal cell-based therapies. Stem Cell Investig. 2022;9:40. https://pmc.ncbi.nlm.nih.gov/articles/PMC9659480/ ↩︎ ↩︎
U.S. FDA. Public Safety Notification on Exosome Products. 2019. https://www.fda.gov/vaccines-blood-biologics/safety-availability-biologics/public-safety-notification-exosome-products ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Sampson S, et al. Platelet-rich plasma: a review of current evidence and clinical applications. J Am Acad Orthop Surg. 2008;16(11):625-635. https://pubmed.ncbi.nlm.nih.gov/19001699/ ↩︎
Drugs.com. (2023). Charcoal, Activated Monograph for Professionals. https://www.drugs.com/monograph/charcoal-activated.html ↩︎ ↩︎