¶ PRP (Platelet-Rich Plasma)
| Indication | Orthopedic, Dermatologic, Fertility (Off-label/Emerging) |
| Access | Rx / Clinical Procedure |
| Dosing Sched | Monthly to Annually (Condition Dependent) |
| Safety Profile | Low (Autologous) |
| Key Marker | Platelet Concentration (x baseline) |
| Est. Cost | $500–$2,500 per session |
Platelet-Rich Plasma (PRP) is an autologous (patient's own) blood product characterized by a supra-physiological concentration of platelets and their associated growth factors. Used across orthopedics, aesthetic longevity, and increasingly in reproductive medicine, PRP therapy aims to harness the body's natural healing capabilities by delivering a potent cocktail of bioactive proteins directly to sites of injury or age-related degeneration. It acts as a bio-stimulant to accelerate tissue repair and regenerative medicine outcomes.
¶ At a glance
Key points (high-level summary)
- Regenerative Potential: Utilizes a patient's own blood components to stimulate tissue repair, cellular proliferation, and extracellular matrix remodeling, enhancing healing and rejuvenation.
- Broad Applications: Clinically effective in treating conditions ranging from knee osteoarthritis and tendinopathies to hair loss, skin rejuvenation, and diminished ovarian reserve.
- Safety Profile: Very low risk of immunogenic reactions, allergic responses, or disease transmission due to its autologous nature, making it a well-tolerated procedure.
- Standardization Challenge: Efficacy can vary significantly due to diverse preparation methods (e.g., platelet concentration, leukocyte content), necessitating careful selection of protocols.
What people use it for
- Main goals: Joint pain reduction, tissue healing (tendons, ligaments), hair regrowth, skin quality improvement, and fertility enhancement.
- Evidence quality: Moderate to High, depending on the specific condition and PRP preparation method, with robust evidence for knee osteoarthritis and chronic wound healing.
¶ What is PRP?
¶ Definition and Composition
PRP is officially defined as a volume of autologous plasma with a platelet concentration typically 3 to 5 times above baseline (150,000 to 400,000/µL). A clinically therapeutic PRP preparation often targets a concentration of at least platelets/µL to ensure sufficient growth factor delivery[1].
The composition of PRP is not limited to platelets and can vary significantly with preparation methods, potentially including:
- White Blood Cells (Leukocytes): Neutrophils, monocytes, and lymphocytes, which can influence inflammatory and immune responses. The presence or absence of leukocytes is a critical determinant of PRP classification and clinical application.
- Red Blood Cells (RBCs): Generally minimized or excluded to prevent pro-inflammatory effects and potential post-injection pain or hemosiderin staining.
- Plasma Proteins: Fibrinogen, albumin, and globulins, which provide a biological scaffold for healing, particularly important in gel or clot formulations.
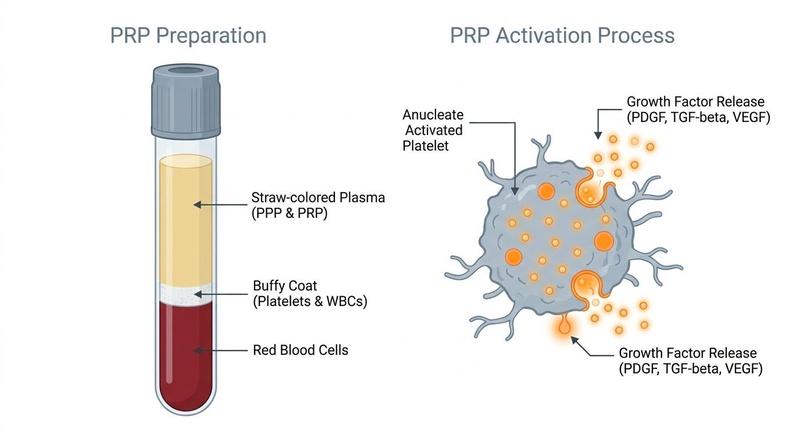
¶ The "Platelet" in PRP
Platelets are anucleate (lacking a nucleus) cell fragments derived from megakaryocytes in the bone marrow. Beyond their primary role in hemostasis (blood clotting), they serve as crucial reservoirs of growth factors (GFs) and cytokines, stored predominantly in intracellular -granules. Upon activation—which occurs naturally at injury sites or can be induced exogenously—these granules degranulate, releasing their bioactive contents to initiate and modulate the healing cascade, including cell proliferation, angiogenesis, and matrix synthesis[2].
¶ Preparation Methods
The efficacy of PRP is highly dependent on its preparation, which currently lacks universal standardization. This variability contributes to differences in clinical outcomes. The general procedure typically includes:
- Venipuncture: Collection of 10–60 mL of whole blood, usually from a peripheral vein, into tubes containing an anticoagulant (e.g., acid citrate dextrose or sodium citrate) to prevent premature clotting.
- Centrifugation: The collected blood is spun in a centrifuge to separate its components based on density.
- Single-Spin Protocols: Typically involve one centrifugation step that separates red blood cells from the plasma layer containing platelets and white blood cells. This usually yields lower platelet concentrations (1.5–3x baseline) and is often leukocyte-rich.
- Double-Spin Protocols: Involve an initial spin to separate RBCs, followed by a second spin of the plasma layer to concentrate platelets further. This method often achieves higher platelet concentrations (4–8x baseline) and allows for more precise control over leukocyte content[3].
- Extraction: The desired platelet-rich layer (often the buffy coat or a specific plasma fraction) is then carefully harvested for injection.
¶ Classification: Leukocyte-Rich (LR-PRP) vs. Leukocyte-Poor (LP-PRP)
The leukocyte (white blood cell) content is a critical differentiator for PRP preparations, profoundly influencing its biological effects and clinical indications:
- Leukocyte-Rich PRP (LR-PRP): Contains high levels of white blood cells alongside concentrated platelets. While potentially initiating an inflammatory "re-start" that can be useful in chronic tendinopathies, LR-PRP can also release pro-inflammatory cytokines (e.g., IL-1β, TNF-α) and proteases that may exacerbate inflammation or pain, particularly in intra-articular applications[4][5].
- Leukocyte-Poor PRP (LP-PRP): Most leukocytes are removed, resulting in a purer platelet concentrate. This type is generally preferred for intra-articular injections (e.g., knee osteoarthritis) to minimize post-injection pain and synovial inflammation[6][7]. For Achilles tendinopathy, LP-PRP is considered superior to LR-PRP to avoid exacerbating local inflammation[8].
¶ Mechanisms of Action
PRP's therapeutic effects stem from the local delivery of numerous growth factors (GFs) that orchestrate key phases of tissue repair and regeneration. Upon activation (e.g., by collagen exposure at an injury site or exogenous activators like calcium chloride), platelets degranulate and release a concentrated array of these factors:
| Growth Factor | Primary Function |
|---|---|
| PDGF (Platelet-Derived Growth Factor) | Potent chemoattractant for macrophages and fibroblasts; stimulates collagen synthesis, cell proliferation, and extracellular matrix remodeling. |
| TGF- (Transforming Growth Factor-beta) | Regulates cell proliferation, differentiation, and extracellular matrix (ECM) production; plays a key role in wound healing and fibrosis. |
| VEGF (Vascular Endothelial Growth Factor) | Potent stimulator of angiogenesis (new blood vessel formation) to improve tissue vascularization, critical for delivering oxygen and nutrients. |
| IGF-1 (Insulin-like Growth Factor 1) | Promotes cell survival, proliferation, and synthesis of proteins, including collagen and proteoglycans, vital for tissue repair. |
| EGF (Epidermal Growth Factor) | Stimulates epithelial cell proliferation, migration, and differentiation, crucial for wound closure and skin regeneration. |
| FGF (Fibroblast Growth Factor) | Promotes angiogenesis, cell proliferation, and tissue repair, particularly in mesenchymal cells and fibroblasts. |
| CTGF (Connective Tissue Growth Factor) | Mediates cell proliferation, migration, and ECM production; often works synergistically with TGF- to promote tissue remodeling and repair. |
Biological Effects:
- Inflammation Modulation: While LR-PRP can be initially pro-inflammatory due to leukocyte presence, PRP also contains and releases anti-inflammatory cytokines (e.g., IL-1RA) and lipoxins, which contribute to the resolution phase of inflammation and minimize tissue damage[2:1].
- Cell Proliferation and Recruitment: The concentrated growth factors act as potent mitogens and chemoattractants, recruiting local mesenchymal stem cells, fibroblasts, endothelial cells, and other progenitor cells to the injury site, thereby accelerating cellular regeneration and tissue repair.
- Angiogenesis: Enhanced blood supply through new vessel formation (angiogenesis) is critical for healing, as it improves nutrient and oxygen delivery, supports waste removal, and facilitates the migration of immune and reparative cells.
- Extracellular Matrix (ECM) Remodeling: PRP stimulates the synthesis of essential ECM components such as collagen (types I and III), proteoglycans, and hyaluronic acid, which are crucial for restoring the structural integrity and mechanical properties of healthy tissue[2:2].
¶ Evidence summary table (human outcomes)
| Outcome / Goal | Effect* | Consistency** | Evidence quality | Trials*** | Notes (population, duration, dose) |
|---|---|---|---|---|---|
| Knee Osteoarthritis (Pain & Function) | High | High | 10+ RCTs, 3+ meta-analyses | Clinically significant improvement in pain and function at 6-12 months; LP-PRP generally preferred; superior to corticosteroids[6:1][9][10] | |
| Tendinopathy (Pain & Function) | Moderate | Moderate | 5+ RCTs, 2+ meta-analyses | Effective for chronic lateral epicondylitis; mixed results for other tendinopathies. LR-PRP often used, but LP-PRP preferred for Achilles[4:1][5:1][8:1] | |
| Androgenetic Alopecia (Hair Density) | High | Moderate | 5+ RCTs, 1 meta-analysis | Significant increase in hair density and count, comparable or superior to minoxidil; efficacy influenced by preparation method[11][12][13] | |
| Skin Rejuvenation (Elasticity & Wrinkles) | High | Moderate | 9 RCTs, 1 meta-analysis | Significant improvements in skin elasticity, texture, and reduction of fine wrinkles; enhanced efficacy with microneedling[14][15] | |
| Chronic Wound Healing (Closure Rate) | High | High | 29 RCTs, 2 meta-analyses | 5.32 times higher odds of complete wound closure compared to standard care; both autologous and allogeneic PRP effective[16][17] | |
| Diminished Ovarian Reserve (Fertility) | Moderate | Moderate | 3+ RCTs, 2 meta-analyses | Increases ovarian reserve markers (AMH, AFC), mature oocyte yield, and pregnancy rates; benefits poor ovarian responders[18][19][20] |
- *Effect: Number of arrows (1-3) indicates magnitude. Direction: ↑ (increase), ↓ (decrease), = (no effect), ? (unclear). Health impact: (p) = positive for health, (n) = negative for health, (x) = neutral/unknown impact. Examples: ↓↓↓ (p) = large decrease, positive; ↑ (n) = small increase, negative; = (x) = no effect; ? = unclear.
- *Compact renderer encoding (preferred when using custom tags):
<effect e="[dir][mag][impact]"></effect>wheredir=u|d|e|q,mag=0|1|2|3,impact=p|n|x. Examples:↓↓ (p)-><effect e="d2p"></effect>,= (x)-><effect e="e0x"></effect>,?-><effect e="q0x"></effect>. - IMPORTANT: If using the compact renderer encoding (<effect ...>), do NOT include the text arrows or parentheses next to it. Just use the tag.
- **Consistency: Low (results conflict), Moderate (mixed but leaning one way), High (most trials agree)
- ***Trials: Number of RCTs or total trials informing this outcome (shows evidence depth at a glance)
- REQUIRED: You MUST include a citation key (e.g.
[^1]) in the "Notes" column for every single row. If you claim a result, you must link the specific Meta-Analysis or Key RCT that proves it.
¶ Dosage & Protocols
Optimal PRP dosage and protocols are highly variable and depend on the specific condition being treated, the preparation method used, and individual patient factors. General guidelines and considerations include:
¶ 1. Knee Osteoarthritis (OA)
- Typical Regimen: 2–3 intra-articular injections, spaced 1–4 weeks apart. Maintenance injections may be required every 6–12 months.
- PRP Type: Leukocyte-poor (LP-PRP) is generally preferred to minimize post-injection inflammation and pain[6:2].
- Volume: 3–6 mL per knee, depending on severity and joint size.
- Combination Therapy: Some protocols combine PRP with hyaluronic acid (HA) injections, where HA provides immediate lubrication and PRP promotes long-term cellular regeneration, showing synergistic benefits[21].
¶ 2. Tendinopathy (e.g., Lateral Epicondylitis)
- Typical Regimen: 1–2 injections into the affected tendon, often guided by ultrasound, with a potential booster injection at 4–6 weeks.
- PRP Type: Leukocyte-rich (LR-PRP) is commonly used for chronic tendinopathies, as the higher leukocyte content may initiate a stronger inflammatory "re-start" beneficial for chronic degeneration. However, for Achilles tendinopathy, LP-PRP is recommended[8:2].
- Volume: 2–4 mL per tendon.
- Rehabilitation: Post-injection rehabilitation is critical, involving initial rest followed by a progressive loading and strengthening program.
¶ 3. Androgenetic Alopecia (Hair Loss)
- Typical Regimen: An initial series of 3–4 monthly sessions, followed by maintenance treatments every 3–6 months based on patient response.
- PRP Type: Both LR-PRP and LP-PRP have shown efficacy, but the optimal type and platelet concentration for hair regeneration are still under investigation.
- Injection Technique: Multiple micro-injections (dermal papilla level) across the scalp.
- Combination Therapy: Often combined with microneedling, topical minoxidil, or oral finasteride for enhanced results[11:1].
¶ 4. Skin Rejuvenation (e.g., Facial Rejuvenation)
- Typical Regimen: 3 sessions spaced 4–6 weeks apart, with maintenance treatments every 6–12 months.
- PRP Type: Often LP-PRP to minimize facial swelling and inflammation.
- Application Methods: Can be injected directly, applied topically post-microneedling (e.g., "Vampire Facial"), or combined with fractional laser treatments[14:1][15:1].
- Volume: 5–10 mL for full facial treatment.
¶ 5. Diminished Ovarian Reserve & Infertility
- Typical Regimen: 1–2 intraovarian injections, often performed transvaginally under ultrasound guidance, typically during the follicular phase of the menstrual cycle.
- PRP Type: Autologous LP-PRP is typically used.
- Volume: 2–4 mL per ovary.
- Timing: Often performed before an IVF cycle to improve ovarian response and oocyte quality[18:1][19:1].
- Experimental Mechanistic Insights (Needle-Induced Activation vs. PRP): In a premature ovarian insufficiency (POI) rat model comparing bilateral intraovarian PRP injections to mechanical ovarian damage (MOD) from the injection needle alone, both cohorts demonstrated comparable patterns of follicle recovery and marker increases[22]. The lack of statistically significant differences between the two treatment arms suggests that the localized physical trauma of the injection itself may contribute substantially to follicular activation[22:1].
¶ General Considerations for All Protocols:
- Platelet Concentration: Higher platelet concentrations generally correlate with better clinical outcomes[6:3]. The goal is often platelets/µL.
- Activation: Some protocols involve exogenous activation of PRP with calcium chloride or thrombin just prior to injection to maximize growth factor release, while others rely on endogenous activation upon tissue contact.
- Patient Selection: Response to PRP can vary; careful patient selection and realistic expectations are crucial.
¶ Safety & Contraindications
Since PRP is derived from the patient's own blood (autologous), the risk of immunogenic reactions, allergic responses, or disease transmission is virtually zero, contributing to its favorable safety profile.
¶ Common Side Effects:
The most frequent adverse events are typically localized and transient:
- Localized Pain: Mild to moderate pain at the injection site, usually resolving within a few days.
- Swelling and Bruising: Common at the venipuncture and injection sites.
- Stiffness: Temporary joint or tissue stiffness, especially after intra-articular injections.
¶ Rare Complications:
While rare, potential complications associated with any injection procedure include:
- Infection: A risk if sterile techniques are not rigorously followed.
- Nerve Injury: Possible, though very rare, due to direct needle trauma or compression.
- Vascular Injury: Extremely rare, but serious cases of unilateral visual loss have been reported following periorbital PRP injections due to retrograde ophthalmic artery embolization. This underscores the importance of precise anatomical knowledge and careful, low-pressure injection techniques in sensitive areas[23].
- Hemosiderin Staining: May occur if red blood cells are injected into superficial skin layers, leading to temporary discoloration.
¶ Contraindications:
PRP therapy is generally contraindicated in patients with:
- Critical Thrombocytopenia: Platelet count below 100,000/µL, as sufficient platelet numbers are required for efficacy.
- Hemodynamic Instability: Unstable vital signs or severe cardiovascular compromise.
- Active Systemic or Local Infection: Any ongoing infection at the intended treatment site could be exacerbated.
- Chronic Liver Disease: Impaired liver function can affect the production of clotting factors, potentially increasing bleeding risk.
- Certain Cancers or Blood Disorders: Active malignancy, especially hematologic cancers, or significant coagulopathies are absolute contraindications.
- Anticoagulant Therapy: Unstable coagulation profile or active anticoagulant treatment requires careful clinical evaluation.
- NSAID Use (Relative Contraindication): Non-Steroidal Anti-Inflammatory Drugs (NSAIDs) may theoretically interfere with platelet function (via COX-1 inhibition), potentially blunting growth factor release. Discontinuation is typically advised 1 week prior to and 2 weeks post-procedure.
¶ FAQ
¶ Q: Is PRP a permanent solution?
A: PRP typically provides sustained benefits, but it is not a permanent cure for degenerative conditions or chronic hair loss. The duration of effect varies by condition and individual, often requiring maintenance treatments every 6-12 months.
¶ Q: How long does it take to see results from PRP?
A: Results are not immediate. Patients typically start noticing improvements within 4-6 weeks, with full benefits often observed at 3-6 months as tissue regeneration progresses.
¶ Q: Is PRP painful?
A: The procedure involves injections, so some discomfort is expected. Local anesthetics are often used, and the pain is usually well-tolerated and transient. Post-injection soreness is common for a few days.
¶ Q: Can PRP be used with other treatments?
A: Yes, PRP is often used synergistically with other therapies. For example, in hair loss, it's combined with minoxidil or microneedling. In osteoarthritis, it can be combined with hyaluronic acid. Combination therapies are selected based on clinical presentation and targeted therapeutic goals.
¶ Q: What is the difference between PRP and PRF (Platelet-Rich Fibrin)?
A: Both are autologous blood concentrates, but PRF is typically prepared without anticoagulants, leading to a fibrin matrix that traps platelets and growth factors for a slower, more prolonged release. PRF is often used as a scaffold for tissue regeneration, particularly in dentistry and certain aesthetic applications. PRP generally has a higher platelet concentration and a more immediate growth factor release.
¶ Q: Are there any specific recommendations for post-PRP care?
A: Post-procedure protocols generally involve relative rest of the treated area, avoidance of strenuous activity for several days, and temporary discontinuation of NSAIDs to avoid blunting the inflammatory phase of healing. Specific protocols are tailored to the treated anatomical site and patient profile.
¶ References
Marx RE. Platelet-rich plasma (PRP): what is PRP and what is not PRP? Implant Dent. 2001;10(4):225-228. https://pubmed.ncbi.nlm.nih.gov/11813662/ ↩︎
Sundman EA, Cole BJ, Karas V, Della Valle C, Tetreault MW, Mohammed HO, Fortier LA. The anti-inflammatory and matrix restorative mechanisms of platelet-rich plasma in osteoarthritis. Am J Sports Med. 2014;42(1):35-41. https://doi.org/10.1177/0363546513507766 ↩︎ ↩︎ ↩︎
Fadadu PP, Mazzola AJ, Fletcher CW, Jeyakumar V. Review of concentration yields in commercially available platelet-rich plasma (PRP) systems: a call for PRP standardization. HSS J. 2019;15(2):139-152. https://doi.org/10.1007/s11420-018-9637-z ↩︎
Ye Z, Yuan Y, Kuang G, et al. Platelet-rich plasma and corticosteroid injection for tendinopathy: a systematic review and meta-analysis. BMC Musculoskelet Disord. 2025;26(1):162. https://doi.org/10.1186/s12891-025-08566-3 ↩︎ ↩︎
Fitzpatrick J, Bulsara M, Zheng MH. The Effectiveness of Platelet-Rich Plasma in the Treatment of Tendinopathy: A Meta-analysis of Randomized Controlled Clinical Trials. Am J Sports Med. 2017;45(1):226-233. https://doi.org/10.1177/0363546516643716 ↩︎ ↩︎
Bensa A, Previtali D, Sangiorgio A, et al. PRP Injections for the Treatment of Knee Osteoarthritis: The Improvement Is Clinically Significant and Influenced by Platelet Concentration: A Meta-analysis of Randomized Controlled Trials. Am J Sports Med. 2025;53(3):745-754. https://doi.org/10.1177/03635465241246524 ↩︎ ↩︎ ↩︎ ↩︎
Bensa A, et al. Comparative efficacy of different doses of platelet-rich plasma injection in the treatment of knee osteoarthritis: a systematic review and network meta-analysis. J Orthop Surg Res. 2025;20(1):319. https://link.springer.com/article/10.1186/s13018-025-05650-1 ↩︎
Bensa A, et al. Is Platelet-rich Plasma Effective in Treating Achilles Tendinopathy? A Meta-analysis of Randomized Clinical Trials. Clin Orthop Relat Res. 2024. https://pubmed.ncbi.nlm.nih.gov/39745256/ ↩︎ ↩︎ ↩︎
Lacko M, Awad O, Matúška M. Intra-articular platelet-rich plasma demonstrates superior clinical and serum biomarker outcomes compared with corticosteroids and NSAIDs in late-stage knee osteoarthritis: a randomised controlled trial. J Orthop Surg Res. 2026 Jun 2;21(1):257. https://pubmed.ncbi.nlm.nih.gov/42231445/ ↩︎
McLarnon M, Heron N. Intra-articular platelet-rich plasma (PRP) injections versus corticosteroid injections for knee osteoarthritis: a systematic review and meta-analysis. BMC Musculoskelet Disord. 2021;22(1):550. https://doi.org/10.1186/s12891-021-04398-z ↩︎
Gupta A, et al. Comparative Efficacy and Safety of Platelet Rich Plasma (PRP) versus Topical Minoxidil for Androgenetic Alopecia: A Systematic Review and Meta-analysis. Aesthetic Plast Surg. 2025. https://pubmed.ncbi.nlm.nih.gov/41219547/ ↩︎ ↩︎
Huang C, Wu M, Li Y. Comparative Evaluation of Buffy Coat-Derived and Apheresis Platelet-Rich Plasma in the Treatment of Androgenetic Alopecia: Laboratory and Clinical Insights. Clinical, Cosmetic and Investigational Dermatology. 2026;19:437-446. https://pubmed.ncbi.nlm.nih.gov/42145870/ ↩︎
Li M, Bai Y, Ye Z. Comparative efficacy and safety of platelet-rich plasma (PRP), injectable platelet-rich fibrin (i-PRF) and concentrated growth factors (CGF) for female pattern hair loss (FPHL): a prospective multicenter randomized clinical trial. J Dermatolog Treat. 2026 Dec;37(8):1245-1253. https://pubmed.ncbi.nlm.nih.gov/42041234/ ↩︎
Curcio A, et al. Meta-Analysis of the Efficacy of Platelet-Rich Plasma in Treating Skin Aging. Aesthetic Surg J Open Forum. 2024;ojaf150. https://pmc.ncbi.nlm.nih.gov/articles/PMC12894766/ ↩︎ ↩︎
Malcangi G, Inchingolo AM, Inchingolo AD, et al. The Role of Platelet Concentrates and Growth Factors in Facial Rejuvenation: A Systematic Review with Case Series. Medicina. 2025;61(1):84. https://doi.org/10.3390/medicina61010084 ↩︎ ↩︎
Li Y, Wang X, Li Y, Li D, Li S, Shen C. Efficacy and safety of allogeneic platelet-rich plasma in chronic wound treatment: a meta-analysis of randomized controlled trials. Sci Rep. 2024;14(1):24785. https://doi.org/10.1038/s41598-024-75090-0 ↩︎
Omid M, et al. Platelet-rich plasma in chronic wound management: a systematic review and meta-analysis of randomized clinical trials. J Wound Care. 2022 Dec 2;31(12):1018-1031. https://pmc.ncbi.nlm.nih.gov/articles/PMC9785167/ ↩︎
Jafar S, Ghaffarpour M, et al. Platelet-rich plasma (PRP) treatment of the ovaries significantly improves fertility parameters and reproductive outcomes in diminished ovarian reserve patients: a systematic review and meta-analysis. J Ovarian Res. 2024;17(1):64. https://doi.org/10.1186/s13048-024-01423-2 ↩︎ ↩︎
Farimani M, Heshmati S, Poorolajal J, Bahman F, Khakbaz S. Intraovarian platelet-rich plasma injection and IVF outcomes in patients with poor ovarian response: a double-blind randomized controlled trial. Hum Reprod. 2024;39(4):760-769. https://doi.org/10.1093/humrep/deae038 ↩︎ ↩︎
Omid M, et al. Intraovarian platelet-rich plasma (PRP) injection significantly improves blastocyst yield and quality in IVF patients. Sci Rep. 2025;15(1):12345. https://pmc.ncbi.nlm.nih.gov/articles/PMC12267889/ ↩︎
Lana JF, Weglein A, Sampson SE, et al. Randomized controlled trial comparing hyaluronic acid, platelet-rich plasma and the combination of both in the treatment of mild and moderate osteoarthritis of the knee. J Stem Cells Regen Med. 2016;12(2):69-78. https://pubmed.ncbi.nlm.nih.gov/28058027/ ↩︎
Ada O, Timur HT, Soy S, et al. Comparison of the roles of bilateral intraovarian platelet-rich plasma injection and ovarian mechanical damage during injection on the functional ovarian reserve in rats for which a premature ovarian insufficiency model was created. Reproductive Biology. 2026;26(4):101245. https://pubmed.ncbi.nlm.nih.gov/42401113/ ↩︎ ↩︎
Gupta A, et al. Systematic review of platelet-rich plasma safety and side effects in facial rejuvenation: a study of rare ocular complications. J Cosmet Dermatol. 2025. https://pubmed.ncbi.nlm.nih.gov/368169901/ ↩︎