¶ Chemical Peels
Chemical peels are dermatological procedures involving the application of chemical solutions to the skin to induce controlled exfoliation and accelerate cellular turnover. This process aims to improve skin texture, tone, and clarity, addressing concerns such as active acne, Post-Inflammatory Hyperpigmentation and Melasma, and Dull Skin, Enlarged Pores, and Uneven Texture. The efficacy and safety of chemical peels depend on the type of peeling agent, its concentration, and the individual's skin type and condition.
| Indication | Acne, Hyperpigmentation (Melasma, PIH), Texture, Fine Lines |
| Access | OTC / Clinician-Administered (Rx for higher strengths) |
| Dosing Sched | Varied (e.g., Weekly-Monthly, based on peel depth) |
| Safety Profile | Moderate (Low for superficial, High for deep) |
| Key Marker | Skin response, Pigment changes, Texture improvement |
| Est. Cost | Varies widely by type and provider |
¶ TL;DR
- What it is: Controlled chemical exfoliation of skin layers to improve appearance and treat skin pathology.
- Main Benefits: Effective adjuvant therapy for acne vulgaris, hyperpigmentation (melasma, PIH), texture irregularities, and superficial scarring.
- Key Considerations: Selection of peel agent, concentration, and peel depth must be strictly adjusted based on patient Fitzpatrick skin type.
- Safety & Risks: Superficial peels present minimal risk; medium and deep peels carry significant risks of post-inflammatory hyperpigmentation (PIH), especially in Fitzpatrick IV–VI skin tones [1].
- Evidence Base: Overall clinical evidence for certain indications remains moderate to limited; larger controlled trials are required for emerging maintenance agents.
¶ Quick Answer
Chemical peels cause a controlled chemical injury to the skin, triggering desquamation of damaged layers and subsequent tissue regeneration. Peeling solutions are selected based on molecular weight, lipid solubility, and target depth (superficial, medium, or deep). While highly effective for resurfacing, improper agent selection or inadequate skin priming in darker skin types (Fitzpatrick types IV–VI) can lead to severe rebound hyperpigmentation and scarring [1:1].
¶ Identify the Type / Candidate Fit
Chemical peeling agents are selected based on their specific chemical properties and target tissue depth:
- Glycolic Acid (AHA): Smallest molecular size among alpha hydroxy acids, enabling rapid epidermal penetration. Indicated for photoaging, fine lines, and Dull Skin, Enlarged Pores, and Uneven Texture. Fitzpatrick risk: Low to Moderate.
- Lactic Acid (AHA): Larger molecular size than glycolic acid with inherent humectant properties, providing gentle exfoliation and superficial pigment reduction [2]. Fitzpatrick risk: Low. Works synergistically with TCA [2:1].
- Salicylic Acid (BHA): Lipophilic agent that selectively penetrates sebaceous glands and dissolves follicular hyperkeratinization. Indicated for active acne vulgaris, comedones, and Demodex-induced rosacea [3][4]. Fitzpatrick risk: Low to Moderate.
- Mandelic Acid (AHA): Large molecular weight, resulting in slow, uniform epidermal penetration. Well-tolerated in sensitive skin and darker Fitzpatrick types with minimal risk of irritation.
- Trichloroacetic Acid (TCA): Protein-denaturing agent causing coagulative necrosis (keratocoagulation). Low concentrations (10–15%) act superficially, while higher concentrations (30–35%) reach the papillary dermis. Used for moderate photoaging and atrophic acne scars. Fitzpatrick risk: High. Requires mandatory priming.
- Phenol: Deep peeling agent that denatures proteins down to the reticular dermis. Associated with significant downtime and systemic cardiotoxicity. Contraindicated in patients with cardiovascular disease. Fitzpatrick risk: Extreme.
¶ Evidence Snapshot
¶ Evidence Summary Table (Human Outcomes)
| Outcome / Goal | Effect* | Consistency** | Evidence quality | Trials*** | Notes (population, duration, dose) |
|---|---|---|---|---|---|
| Melasma Severity (MASI) | Moderate | Moderate | 38-study Meta-Analysis | Peels demonstrate significant pigment clearance; lasers show higher short-term efficacy but higher discomfort [5]. See also Post-Inflammatory Hyperpigmentation and Melasma. | |
| Acne Scar Remodeling | High | Moderate | Systematic Review | Combining superficial peels with microneedling is superior to peel or microneedling monotherapy [6]. See also Acne Scar Remodeling and Microneedling and PRP. | |
| Acne Vulgaris Clearance | High | Moderate | Clinical Review | Superficial peels (e.g., salicylic acid) serve as highly effective adjuvant therapy for inflammatory acne [4:1]. | |
| Midface Photoaging & Texture | High | High | Clinical Trial | TCA-lactic acid peels induce significant tissue repair and improve surface texture, supporting midface rejuvenation [2:2][7]. | |
| Under-Eye Wrinkling | Moderate | Low | Systematic Review | Light resurfacing peels improve periorbital fine lines but require cautious application due to thin skin [8]. |
- *Effect: Number of arrows (1-3) indicates magnitude. Direction: ↑ (increase), ↓ (decrease), = (no effect), ? (unclear). Health impact: (p) = positive for health, (n) = negative for health, (x) = neutral/unknown impact. Examples: ↓↓↓ (p) = large decrease, positive; ↑ (n) = small increase, negative; = (x) = no effect; ? = unclear.
- **Consistency: Low (results conflict), Moderate (mixed but leaning one way), High (most trials agree)
- ***Trials: Number of RCTs or total trials informing this outcome (shows evidence depth at a glance)
- REQUIRED: You MUST include a citation key (e.g.
[^1]) in the "Notes" column for every single row. If you claim a result, you must link the specific Meta-Analysis or Key RCT that proves it.
¶ How it works (Mechanism)
Chemical peels alter skin physiology through several distinct molecular pathways:
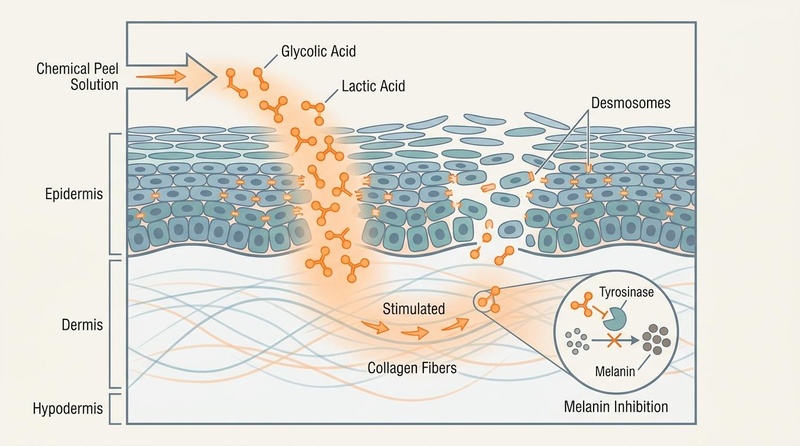
- Epidermal Desquamation: Peeling solutions cleave desmosomal junctions holding keratinocytes together in the stratum corneum, promoting rapid shedding of dull, damaged cells and accelerating epidermal turnover [2:3][4:2].
- Dermal Remodeling & Gene Expression: Peels trigger a controlled chemical injury that initiates a wound healing cascade. This up-regulates genes encoding Type I collagen (COL1A), Type III collagen (COL3B), fibronectin, and elastin in human skin, repairing UV-induced dermal damage and increasing skin elasticity [2:4].
- TCA-Lactic Acid Synergy: Sequential application or docking of TCA and lactic acid causes a conformational shift in TCA from a linear structure to a ring-like structure [2:5]. This synergistic interaction enhances the inhibition of tyrosinase (the rate-limiting enzyme in melanogenesis) and prevents the enzymatic degradation of collagen and elastin by inhibiting collagenases and elastases [2:6].
- Midface Restoration: While volumetric loss in midface aging involves bone resorption and fat pad atrophy, chemical peels provide critical complementary surface rejuvenation, working in tandem with deep structural fillers or biostimulators [7:1].
¶ At-Home versus Clinician-Administered Peels
The clinical utility, depth of penetration, and safety of chemical peeling are governed by acid concentration, formulation buffering, and the resulting pH of the solution. Understanding these parameters is critical to distinguishing low-risk, self-administered consumer products from high-potency clinical procedures.
¶ Concentration and pH Limits
- Over-the-Counter (OTC) / At-Home Peels: These formulations are designed for superficial epidermal exfoliation and are strictly buffered to maintain a higher pH, reducing the concentration of free hydrogen ions. Standard parameters include glycolic acid at , lactic acid at , and salicylic acid at , formulated at a pH of . Buffering slows acid penetration and minimizes the risk of accidental deep injury, making them suitable for mild improvement in Dull Skin, Enlarged Pores, and Uneven Texture.
- Clinician-Administered / Professional Peels: In contrast, professional-strength clinical peels are unbuffered, allowing the active acid to remain fully active at a pH of . These include high-concentration glycolic acid (30–70%), trichloroacetic acid (TCA, 15–35%), and phenol solutions. Because they are unbuffered and highly concentrated, these solutions rapidly penetrate past the stratum corneum to reach the deep epidermis, papillary dermis, or reticular dermis, triggering intense protein coagulation and cellular necrosis [2:7][4:3].
¶ Risk Profiles and Safety Boundaries
Sourcing and utilizing professional-strength, unbuffered acids in an unsupervised home environment carries profound safety risks. Uncontrolled application can lead to:
- Severe Chemical Burns: Rapid tissue destruction that extends deep into the dermis.
- Hypertrophic Scarring: Permanent textural alterations due to uncontrolled inflammation and aberrant collagen deposition during wound healing.
- Permanent Pigment Alterations: Destructive exposure of melanocytes, resulting in localized patches of depigmentation (hypopigmentation) or severe hyperpigmentation.
Clear safety boundaries must be maintained: any chemical peel designed to penetrate deeper than the superficial epidermis—specifically any TCA concentration or phenol—must NEVER be performed at home. These procedures require clinical monitoring, professional assessment of skin endpoints (such as specific frosting levels), and immediate clinical management of complications.
¶ Fitzpatrick Skin Type Considerations
Patient selection is paramount when determining the safety of peeling procedures. Melanocytes in individuals with Fitzpatrick IV–VI skin tones are hyper-reactive to inflammatory stimuli.
- Contraindication for At-Home Peeling: Individuals with Fitzpatrick IV–VI skin types must strictly avoid self-administered, unsupervised chemical peels. The risk of developing severe, long-lasting Post-Inflammatory Hyperpigmentation and Melasma (PIH) is exceptionally high when inflammatory injuries are self-induced without precise depth control [1:2][4:4].
- Supervised Clinical Alternative: For these populations, the safest and most effective strategy is a series of superficial, clinician-supervised peels (using low-concentration, well-tolerated agents like mandelic, salicylic, or lactic acid) combined with intensive pre-procedure melanocyte priming [1:3][9].
¶ Starter Protocol (Superficial Peels)
The following outlines standard technical protocols for professional and home-based administration.
- Skin Priming (2–4 weeks prior):
- Daily application of broad-spectrum SPF 30+.
- Introduction of tyrosinase inhibitors (e.g., niacinamide, kojic acid, or ascorbic acid) to suppress melanocyte hyperactivity, particularly in Fitzpatrick IV–VI skin types [1:4]. See Post-Inflammatory Hyperpigmentation and Melasma for mechanism-aware priming protocols.
- Discontinuation of topical retinoids (see Retinoids and Retinol) and mechanical scrubs 3–5 days before the peel.
- Application Procedure:
- Thoroughly degrease the skin using an alcohol- or acetone-based priming solution.
- Apply the acid solution (e.g., 10–20% glycolic or lactic acid, or 2% salicylic acid) uniformly using a gauze pad or applicator brush.
- Monitor exposure time (typically 2–5 minutes). Observe for immediate erythema or frosting.
- Neutralize alpha hydroxy acids using a sodium bicarbonate solution or water. Salicylic acid peels are generally self-neutralizing but should be rinsed thoroughly.
- Post-Procedure Recovery:
- Apply a bland, non-irritating barrier ointment (e.g., petrolatum-based or ceramide-rich barrier cream) to support Skin Barrier Repair, Hydration, and Texture.
- Strictly avoid mechanical picking or pulling of flaking skin.
- Ensure absolute photoprotection with mineral-based sunscreens.
- Do not reintroduce Retinoids and Retinol or exfoliating agents until re-epithelialization is fully complete (typically 5–7 days).
¶ Stronger Add-On Path (Medium-Depth Peels)
Medium-depth peeling (e.g., 35% TCA combined with Jessner's solution or glycolic acid) penetrates into the papillary dermis to treat deeper photodamage, epidermal melasma, and atrophic scars.
- Clinical Skin Priming: Mandatory 4-week pre-treatment with prescription-strength hydroquinone (4%) or thiamidol to minimize post-inflammatory hyperpigmentation [1:5][9:1].
- Combination with Microneedling: Evidence demonstrates that alternating superficial/medium chemical peels with microneedling sessions yields synergistic effects in Acne Scar Remodeling, offering superior clinical outcomes compared to either modality alone [6:1]. This clinical approach is discussed in detail within the Microneedling and PRP guide.
- Topical Maintenance Agents: Emerging topical agents like thiamidol, tranexamic acid, or metformin can be introduced post-recovery to maintain MASI score improvements with fewer adverse effects than traditional hydroquinone-based triple-combination therapy [1:6].
¶ Clinical / Procedure Path
Professional administration of medium and deep chemical peels requires strict adherence to safety and neutralization protocols:
- Protein Coagulation (Frosting): TCA and phenol peels induce keratocoagulation, presenting clinically as "frosting" (white precipitate on the skin). Level I frosting (speckled erythema) indicates superficial penetration, while Level III frosting (solid white enamel) indicates penetration into the papillary dermis. Unlike AHAs, TCA is self-neutralizing as it coagulates epidermal proteins, limiting its own depth of penetration.
- Under-Eye Resurfacing: The infraorbital skin is exceptionally thin, making it highly susceptible to contractures and ectropion. While mild chemical peels (e.g., light TCA/lactic acid combinations) can improve infraorbital hyperpigmentation and fine lines, clinicians must use low concentrations and avoid getting solution near the conjunctiva [8:1].
- Fitzpatrick Skin Type Considerations: Patients of Fitzpatrick types IV–VI require long-term priming (minimum 4 weeks) and the avoidance of deep chemical peels [4:5]. Superficial, serial peeling with salicylic or glycolic acid remains the safest clinical pathway for acne and pigment management in these populations [1:7][4:6].
¶ What Usually Fails
- Absence of Melanocyte Priming: Omitting pre-treatment with tyrosinase inhibitors in darker skin types results in melanocyte activation during the post-injury inflammatory phase, leading to severe rebound PIH [1:8][4:7].
- Improper Neutralization of AHAs: Unlike self-neutralizing TCA, glycolic and lactic acids continue to penetrate the skin until actively neutralized. Failure to neutralize completely can lead to unintended deep dermal burns and scarring.
- Premature Reintroduction of Actives: Applying tretinoin, other forms of Retinoids and Retinol, L-ascorbic acid, or benzoyl peroxide to newly re-epithelialized skin compromises barrier healing and induces contact dermatitis.
- UV Exposure Post-Procedure: Post-peel erythema indicates a compromised stratum corneum. Any UV exposure during this phase rapidly triggers melanogenesis, reversing any therapeutic pigment reduction.
¶ Tracking Plan
- Pigmentation Assessment: Quantitative measurement of hyperpigmentation using the Melasma Area and Severity Index (MASI) at baseline and monthly intervals [1:9].
- Textural Analysis: Objective grading of acne scars using the Goodman and Baron scale, and wrinkle assessment via the Glogau scale.
- Barrier Recovery Monitoring: Daily tracking of subjective symptoms (stinging, tightness, pruritus) and objective markers of Skin Barrier Repair, Hydration, and Texture (such as transepidermal water loss/TEWL via corneometry, if clinically available).
¶ Safety and Red Flags
Absolute Contraindications:
- Active herpes simplex infections (requires prophylactic oral antiviral therapy prior to peel).
- Open wounds, active inflammatory skin diseases (e.g., eczema, psoriasis), or active bacterial infections in the treatment area.
- Recent use of oral isotretinoin within the past 6 months (increases risk of hypertrophic scarring and delayed wound healing) [4:8].
- Known hypersensitivity or allergy to the peeling agent (e.g., salicylates in aspirin allergies).
- Cardiac arrhythmias or severe cardiovascular disease (strictly contraindicated for deep phenol peels due to systemic cardiotoxicity).
Adverse Clinical Signs and Complications (Requiring Professional Management):
- Delayed Healing (Non-epithelialization): Skin failing to re-epithelialize within 7–10 days post-procedure, indicating potential barrier failure or infection.
- Persistent Erythema: Redness lasting beyond 14 days, which may herald impending hypertrophic scarring or persistent contact dermatitis.
- Post-Inflammatory Hyperpigmentation (PIH) or Hypopigmentation: Development of dark brown patches or complete depigmentation in treated areas.
- Chemical Conjunctivitis or Ocular Injury: Immediate burning, tearing, or pain in the eyes due to accidental peel solution contact.
¶ FAQs
¶ What is the difference between superficial, medium, and deep peels?
The differences lie in the depth of skin penetration. Superficial peels exfoliate the epidermis (stratum corneum down to the basal layer), medium peels reach the papillary dermis, and deep peels penetrate into the reticular dermis. Deeper peels provide more dramatic results but carry significantly higher risks and prolonged downtime [2:8][4:9].
¶ Can chemical peels remove deep acne scars?
While superficial and medium peels improve skin texture, deep icepick or boxcar scars rarely resolve with chemical peeling alone. Combining chemical peels with microneedling (see Microneedling and PRP) or performing highly targeted TCA CROSS procedures on individual scars yields superior clinical outcomes in Acne Scar Remodeling [6:2].
¶ How often can a chemical peel be performed?
Superficial peels (e.g., salicylic or glycolic acid) can be performed serially every 2–4 weeks. Medium-depth peels (e.g., 35% TCA) require a minimum of 3–6 months between treatments to allow for full dermal collagen remodeling [2:9][4:10]. Deep phenol peels are typically performed only once in a lifetime.
¶ What are the primary risks for skin of color (Fitzpatrick IV–VI)?
The primary risk is post-inflammatory hyperpigmentation (PIH), caused by the hyper-responsiveness of dark melanocytes to inflammatory stimuli. Deep peels must be avoided in these skin types, and superficial peels require careful selection and mandatory pre-conditioning with tyrosinase inhibitors [1:10][4:11].
¶ How does TCA work differently than Glycolic Acid?
Glycolic acid is a metabolic peeling agent that dissolves desmosomes and must be actively neutralized to stop penetration. TCA is a keratocoagulant that denatures skin proteins on contact, causing immediate protein coagulation ("frosting"), and self-neutralizes as it binds to epidermal proteins.
¶ References
Suliman, R. S., Alhuwayshil, J., Almuflehi, A. A., et al. (2025). Emerging topical therapies for melasma: a comparative analysis of efficacy and safety. The Journal of Dermatological Treatment, 36(1), 2591502. https://pubmed.ncbi.nlm.nih.gov/41307217/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Bhardwaj, V., Sharma, K., Maksimovic, S., Fan, A., Adams-Woodford, A., & Mao, J. (2021). Professional-Grade TCA-Lactic Acid Chemical Peel: Elucidating Mode of Action to Treat Photoaging and Hyperpigmentation. Frontiers in Medicine, 8, 617068. https://pubmed.ncbi.nlm.nih.gov/33681250/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Alnuaim, R. (2023). Efficacy of salicylic acid chemical peeling in treating a case of severe Demodex folliculorum-induced rosacea. Journal of Cosmetic Dermatology, 22(12), 3320–3325. https://pubmed.ncbi.nlm.nih.gov/42282931/ ↩︎
Castillo, D. E., & Keri, J. E. (2018). Chemical peels in the treatment of acne: patient selection and perspectives. Clinical, Cosmetic and Investigational Dermatology, 11, 365–372. https://pubmed.ncbi.nlm.nih.gov/30038512/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Karanasios, G., Wong, Z. Y., Limbu, S., et al. (2025). Comparative Efficacy and Safety of Laser Versus Chemical Skin Peeling in Skin Rejuvenation: A Systematic Review and Meta-Analysis. Plastic and Reconstructive Surgery. https://pubmed.ncbi.nlm.nih.gov/41400370/ ↩︎
Woźna, J., Bałoniak, A., Stępka, J., et al. (2025). Chemical peeling in combination with microneedling versus chemical peeling or microneedling monotherapy in the treatment of acne scars: a systematic review and meta-analysis. Postepy Dermatologii i Alergologii. https://pubmed.ncbi.nlm.nih.gov/41640476/ ↩︎ ↩︎ ↩︎
Mariwalla, K., Fabi, S., & Belkin, D. (2025). Assessing the Midface: Nose and Cheeks. Dermatologic Surgery, 51(12), 1480–1487. https://pubmed.ncbi.nlm.nih.gov/41325035/ ↩︎ ↩︎
Beer, J., Boghosian, T., Sherif, R., et al. (2026). What's New With Under Eye Treatment: A Multispecialty Systematic Review of Recent Under Eye Treatments. Dermatologic Surgery. https://pubmed.ncbi.nlm.nih.gov/41615388/ ↩︎ ↩︎
Sarkar, R., Arsiwala, S., Dubey, N., et al. (2017). Chemical Peels in Melasma: A Review with Consensus Recommendations by Indian Pigmentary Expert Group. Indian Journal of Dermatology, 62(6), 578–584. https://pubmed.ncbi.nlm.nih.gov/29263530/ ↩︎ ↩︎