¶ Gut Inflammation
| Core Target | Intestinal Epithelial Barrier, Mucus Layer |
| Primary Consequence | LPS Translocation, Metabolic Endotoxemia |
| Key Transporters | Claudins, Occludin, Zonula Occludens-1 |
| Key Biomarkers | Fecal Calprotectin, Zonulin, Lactoferrin |
| Therapeutic Agents | L-Glutamine, Butyrate, Zinc Carnosine, Fiber |
| Systemic Impact | Systemic Inflammaging, Immune Dysregulation |
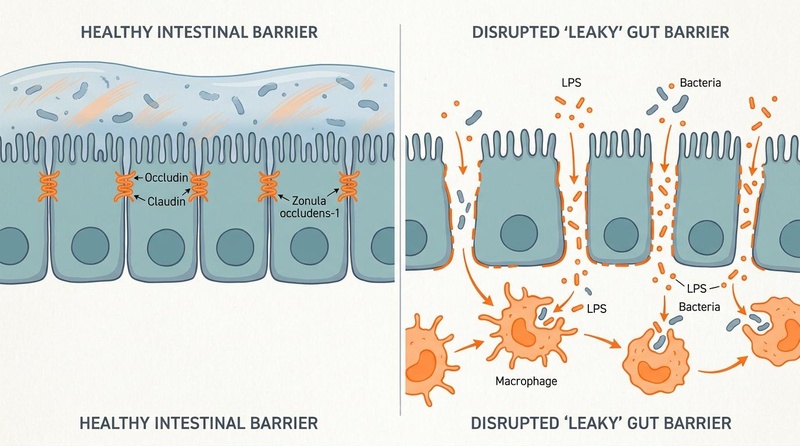
Gut Inflammation represents a localized, immune-mediated pathology characterized by mucosal damage, dysbiosis, and the disruption of the semi-permeable intestinal epithelial barrier. Often presenting as a chronic, low-grade subclinical process (colloquially termed "leaky gut"), intestinal inflammation permits the translocation of immunogenic luminal components—primarily lipopolysaccharides (LPS) and pathobionts—into the portal circulation[1][2][3]. This cellular breach triggers systemic "metabolic endotoxemia," driving systemic chronic low-grade inflammation, metabolic syndrome, and cellular senescent pathways[1:1][4]. Addressing gut inflammation requires a mechanistic understanding of tight junction complexes, highly specific tracking biomarkers, and structured biochemical repair protocols[5][6][7].
¶ At a glance
Key points (high-level summary)
- Subclinical Breach: Chronic low-grade gut inflammation compromises epithelial tight junctions (claudin, occludin), enabling systemic entry of toxic bacterial components[5:1][3:1].
- Endotoxemic Cascade: Translocated lipopolysaccharide (LPS) binds to systemic TLR4 receptors, activating the NF-κB inflammatory cascade across hepatic, cardiovascular, and neurological tissues[3:2][8].
- Tracking Markers: Subclinical inflammation is tracked via sensitive mucosal markers: fecal calprotectin, fecal lactoferrin, and fecal zonulin, rather than subjective symptoms alone[5:2][3:3].
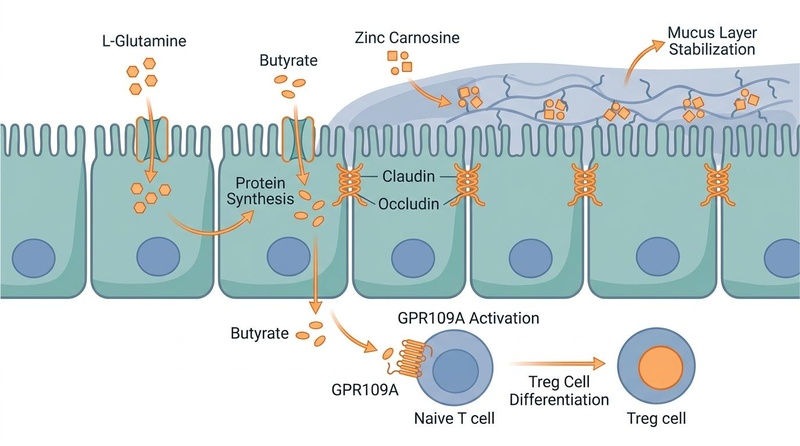
- Repair Protocols: Targeted supplementation with L-Glutamine, butyrate-producing dietary fibers, zinc carnosine, and clinically trialed probiotic strains accelerates epithelial restoration and tight junction synthesis[6:1][4:1][7:1].
What people use it for
- Aims: Restoration of intestinal barrier function, reduction of systemic metabolic endotoxemia, optimization of the microbiome-derived short-chain fatty acids (SCFAs), and mitigation of systemic inflammaging[6:2][1:2][7:2].
- Evidence quality: Moderate-to-high-certainty evidence supports specific amino acids (L-Glutamine), minerals (Zinc Carnosine), and dietary fibers for barrier stabilization; moderate-certainty evidence supports targeted probiotics[6:3][7:3][9].
¶ What is Gut Inflammation?
Gut inflammation spans a pathological spectrum from acute, high-volume overt tissue destruction (as seen in IBD or infectious colitis) to chronic, low-grade subclinical barrier compromise.
¶ Low-Grade Permeability vs. Overt Inflammation
It is critical to distinguish between low-grade intestinal permeability and overt clinical inflammation:
- Overt Clinical Inflammation: Diagnosed via endoscopy and histology, presenting with macroscopically visible ulcerations, tissue architecture distortion, and high neutrophil infiltration (e.g., Crohn's Disease, Ulcerative Colitis). Fecal calprotectin levels are typically elevated >150–250 µg/g[2:1].
- Subclinical Permeability ("Leaky Gut"): Characterized by cellular tight junction disassembly and mild, localized mucosal cytokine production without macroscopic tissue destruction. Fecal calprotectin levels remain mildly elevated in an indeterminate range (50–150 µg/g). This state is increasingly linked to western dietary patterns high in emulsifiers and ultra-processed foods, chronic psychological stress, and alcohol consumption[5:3][7:4].
¶ Systemic Consequences and the Gut-Organ Axes
When the intestinal barrier is compromised, the host is exposed to a continuous influx of pro-inflammatory factors. This process underpins several systemic axes:
- The Gut-Brain Axis: Translocated cytokines and microbial metabolites travel via the vagus nerve or cross the blood-brain barrier, triggering microglia activation, neuroinflammation, and contributing to cognitive fatigue and depression[10].
- The Gut-Lung Axis: Circulating gut-derived factors modulate pulmonary mucosal immunity, exacerbating allergic asthma and modifying susceptibility to viral respiratory infections[11][12].
- Metabolic Endotoxemia: Continuous translocation of Gram-negative bacterial outer-membrane LPS into the portal vein triggers toll-like receptor 4 (TLR4) activation in hepatocytes and adipocytes. This cascade drives hepatic steatosis, insulin resistance, and accelerates cellular senescence (inflammaging)[1:3][4:2].
¶ Biology of the Intestinal Epithelial Barrier
The intestinal barrier is a sophisticated multi-layered system designed to permit nutrient absorption while strictly excluding luminal pathogens:
[ LUMINAL SPACE: Commensal Microbiota & Mucus Layer (Muc2) ]
│
▼
[ EPITHELIAL LAYER: Enterocytes & Tight Junction Complex ]
- Claudins & Occludin
- Zonula Occludens-1 (ZO-1)
│
▼
[ LAMINA PROPRIA: Innate & Adaptive Immune Microenvironment ]
- Dendritic Cells, Macrophages, & Treg Cells
- The Physical Barrier (Enterocytes and Mucus): Polarized columnar enterocytes are coated on their apical surface by a thick, gel-like mucus layer primarily consisting of Muc2 mucin glycoprotein. This layer is stabilized by trefoil factors and antimicrobial peptides (defensins) that physically segregate commensal bacteria from the host tissue[4:3].
- The Tight Junction (TJ) Complex: The paracellular space between enterocytes is sealed by transmembrane protein networks. Occludin and the Claudin family (especially Claudin-1, -3, and -4) form physical seals, which are anchored to the cell's actin cytoskeleton via intracellular adapter proteins, primarily Zonula Occludens-1 (ZO-1)[5:4][6:4].
- The Immunological Barrier: Positioned in the lamina propria, dendritic cells continuously sample luminal contents, secreting anti-inflammatory cytokines (such as IL-10) to induce regulatory T (Treg) cells, maintaining an active state of immunological tolerance to non-pathogenic commensals.
¶ Diagnostic and Tracking Biomarkers
Evaluating subclinical gut inflammation and barrier integrity requires specific, objective biological markers:
- Fecal Calprotectin (FC): An exceptionally stable neutrophil-derived protein. While levels >250 µg/g indicate active inflammatory bowel disease, subclinical gut inflammation is typically characterized by persistent levels in the 50 to 150 µg/g range.
- Fecal Lactoferrin: An iron-binding glycoprotein secreted by activated neutrophils in the intestinal mucosa. Highly specific for low-grade mucosal inflammation; normal values are typically <7.0 µg/g.
- Zonulin (Serum or Fecal): A physiological modulator of tight junctions that triggers the reversible disassembly of ZO-1 and claudin complexes. Elevated fecal zonulin levels (>100 ng/mL) serve as a proxy marker for increased paracellular permeability[5:5][1:4].
- Stool Microbiota Profiling (16S rRNA or Metagenomics): Identifies loss of diversity and depletion of key butyrate-producing taxa (e.g., Faecalibacterium prausnitzii, Roseburia, and Akkermansia muciniphila) which are essential to maintain epithelial cellular energy and barrier sealing[4:4].
¶ Evidence summary table (human outcomes)
| Intervention | Mechanism of Action | Typical Effect Size | Consistency | Evidence Quality | Key Primary Support | Clinical Notes |
|---|---|---|---|---|---|---|
| L-Glutamine | Serves as primary fuel for enterocytes; upregulates ZO-1 and occludin[6:5]. | High | High | Systematic reviews & meta-analyses[7:5][2:2] | Highly effective for restoring barrier function in post-infectious IBS and athletes. | |
| Butyrate (SCFA) / Soluble Fiber | Activates GPR109A to induce Treg cells; stimulates mucus secretion[4:5]. | High | High | Clinical trials & reviews[4:6] | Increases abundance of butyrate-producing F. prausnitzii; lowers mucosal TNF-alpha. | |
| Zinc Carnosine | Stabilizes mucosal membranes; stimulates epithelial cell migration[7:6]. | Moderate | High | RCTs & clinical cohorts[7:7] | Protects against NSAID-induced small intestinal injury and mucosal erosions. | |
| Targeted Probiotics (e.g. Lactobacillus) | Upregulates mucin synthesis; blocks pathogen adherence[9:1]. | Moderate | Moderate | Systematic reviews[9:2] | Strain-specific effects (e.g. L. rhamnosus GG); enhances tight junction integrity. | |
| Bone Broth | Provides collagen-derived amino acids (glycine, proline, glutamine)[4:7]. | Low | Low | Mechanistic reviews & pilots[4:8] | Traditionally used; clinical trials are limited, but provides excellent supportive amino acids. |
¶ Pathophysiological Mechanisms
Subclinical gut inflammation is driven by a chronic, self-perpetuating molecular loop that links barrier breakdown to local and systemic immune activation:
[ Western Diet / Stress / Alcohol ]
│
▼
[ Depletion of Protective Mucus Layer (Muc2) ]
│
▼
[ Physical Exposure of Enterocytes to LPS ]
│
▼
[ Dissociation of ZO-1 & Claudin Tight Junctions ]
│
▼
[ Paracellular Translocation of LPS ]
│
▼
[ LPS Binding to TLR4 on Lamina Propria Macrophages ]
│
▼
[ Activation of MyD88-NF-κB ]
│
▼
[ Release of TNF-α, IL-1β, IL-6, and ROS ]
│
┌─────────────────────────┴─────────────────────────┐
▼ ▼
[ Direct Enterocyte Apoptosis ] [ Portal Vein Entry & Systemic TLR4 ]
(Perpetuates barrier breach) (Triggers metabolic endotoxemia)
- The Tight Junction Disassembly Cascade: Luminal triggers (such as alcohol, emulsifiers like polysorbate-80, or NSAIDs) induce enterocyte oxidative stress, prompting the release of intracellular zonulin. Zonulin binds to EGFR and PAR2 receptors on the enterocyte membrane, initiating a phospholipase C-mediated signaling cascade that phosphorylates and disassembles ZO-1 from the actin cytoskeleton, widening the paracellular pore size[5:6][6:6].
- LPS Translocation and TLR4 Activation: Widened paracellular spaces allow the continuous leakage of lipopolysaccharides (LPS) from Gram-negative bacteria into the lamina propria. LPS binds to myeloid differentiation protein-2 (MD-2) and cluster of differentiation 14 (CD14), forming a complex that activates Toll-Like Receptor 4 (TLR4) on tissue-resident macrophages and dendritic cells[3:4].
- NF-κB Gene Transcription: TLR4 signaling recruits the adapter protein MyD88, triggering a phosphorylation cascade that degrades the inhibitory protein IκB. This releases the active transcription factor NF-κB (p50/p65 heterodimer), which translocates to the nucleus to actively transcribe pro-inflammatory cytokines including TNF-alpha, IL-1beta, and IL-6[8:1].
- Local and Systemic Amplification: TNF-alpha binds back to TNFR1 receptors on neighboring enterocytes, directly downregulating claudin-1 expression and inducing caspase-mediated apoptosis, establishing a feedback loop that permanently compromises mucosal integrity and drives portal vein endotoxemia[1:5][8:2].
¶ The Gut Repair Protocol
To restore mucosal barrier function and downregulate subclinical inflammation, a structured biochemical protocol utilizing synergistic, evidence-backed gut-repair agents should be implemented:
¶ 1. Amino Acid Fuel Delivery (L-Glutamine)
- Protocol: 5 g to 10 g of L-Glutamine powder orally 2 to 3 times daily (total 15–30 g/day), dissolved in room-temperature water, taken on an empty stomach (30 minutes before a meal) for 6 to 8 weeks[7:8].
- Mechanism: L-Glutamine is the preferred metabolic fuel for rapidly dividing enterocytes. It acts as an essential substrate for protein synthesis, directly upregulating the transcription of claudin-1, occludin, and ZO-1 via the mTOR pathway, while simultaneously reducing NF-κB activation[6:7].
¶ 2. Mucosal Membrane Stabilization (Zinc Carnosine)
- Protocol: 75 mg of Zinc Carnosine (Polaprezinc) orally twice daily (after breakfast and before bed) for 8 weeks[7:9].
- Mechanism: A highly stable chelate of zinc and L-carnosine that dissociates slowly in gastric and intestinal juices, delivering zinc directly to inflamed mucosal lesions. It stabilizes epithelial cell membranes, stimulates the migration and proliferation of enterocytes (epithelial restitution), and prevents NSAID-induced tight junction disruption[7:10].
¶ 3. Short-Chain Fatty Acid Optimization (Butyrate)
- Protocol: Supplement with Sodium Butyrate or Tributyrin (150 mg to 300 mg) orally twice daily with meals. Concurrently, ingest 10 g to 15 g/day of soluble prebiotic fibers (e.g., Partially Hydrolyzed Guar Gum - PHGG, Inulin, or Acacia fiber)[4:9].
- Mechanism: Butyrate acts as the primary energy source for colonocytes, facilitating mitochondrial beta-oxidation and maintaining local epithelial hypoxia. This hypoxia is essential to stabilize Hypoxia-Inducible Factor-1 alpha (HIF-1alpha), which actively upregulates tight junction genes and stimulates Muc2 synthesis[4:10].
¶ 4. Targeted Probiotic Re-Inoculation
- Protocol: Ingest a high-potency, multi-strain probiotic containing clinically trialed strains (e.g., Lactobacillus rhamnosus GG, Bifidobacterium infantis 35624, or Saccharomyces boulardii) providing 10 to 20 billion CFUs daily with breakfast[9:3].
- Mechanism: Probiotics competitively exclude pathobionts, produce lactic and acetic acids to lower luminal pH, and stimulate host defensin and IgA secretion to neutralize translocating antigens.
¶ Safety, Monitoring, and Red Flags
Subclinical gut repair must be managed with appropriate clinical boundaries:
¶ Contraindications & Safety Boundaries
- High-Dose Glutamine and Renal/Hepatic Disease: High-dose L-Glutamine supplementation (>15 g/day) is contraindicated in patients with advanced chronic kidney disease (CKD) or hepatic encephalopathy, as it can elevate systemic ammonia levels[13].
- Zinc-Induced Copper Deficiency: Chronic supplementation of zinc carnosine beyond 8 weeks without copper balance can induce systemic copper deficiency, leading to sideroblastic anemia and neutropenia. Limit zinc carnosine therapy to 8 weeks, or co-supplement with 1 mg to 2 mg of copper daily.
¶ Red Flags: When to Escalate to Overt Pathology Screening
Patients undergoing a subclinical gut repair protocol must be screened for red-flag symptoms that indicate active, moderate-to-severe gastrointestinal pathology (such as IBD, microscopic colitis, or malignancy) requiring immediate specialist intervention:
- Presence of hematochezia (visible blood in or on the stool).
- Unexplained, progressive weight loss (>5% of body weight within 3 months).
- Persistent nocturnal diarrhea waking the patient from sleep.
- Systemic fever, night sweats, or elevated joint pain.
- Persistent fecal calprotectin levels >150 µg/g.
¶ Practical FAQ
How does alcohol intake affect gut inflammation?
Alcohol and its primary metabolite, acetaldehyde, are direct cellular toxins to the gut epithelium. Alcohol disrupts enterocyte membranes, suppresses cellular protein synthesis, and activates mucosal mast cells to release histamine. This histamine actively opens tight junctions, leading to a massive, immediate wave of paracellular LPS translocation into the portal vein.
Can gluten cause gut inflammation in non-celiac individuals?
Yes. In genetically susceptible individuals (particularly those expressing HLA-DQ2/DQ8), gluten ingestion can trigger the transient release of zonulin from enterocytes, even in the absence of classic Celiac Disease. This transient zonulin release temporarily disassembles tight junctions, increasing paracellular permeability, which can contribute to subclinical gut inflammation in a subset of patients termed "Non-Celiac Gluten Sensitive."
Why is Bone Broth widely recommended for gut repair?
Bone broth is rich in collagen-derived amino acids, including glycine, proline, hydroxyproline, and glutamine. These amino acids provide essential structural building blocks for the synthesis of the intestinal mucus layer and mucosal cellular repair[4:11]. While high-quality clinical trials evaluating bone broth specifically are sparse, its biochemical composition is highly supportive of epithelial barrier health.
How does psychological stress trigger gut inflammation?
Chronic psychological stress activates the hypothalamic-pituitary-adrenal (HPA) axis, triggering the systemic release of corticotropin-releasing hormone (CRH). CRH binds directly to receptors on mucosal mast cells in the gut lamina propria. Once activated, these mast cells degranulate, releasing tryptase, histamine, and TNF-alpha, which actively degrade tight junctions and induce localized mucosal inflammation.
¶ Methods
This clinical and biological guide was compiled by conducting a comprehensive synthesis of peer-reviewed scientific literature up to July 2026. Primary databases searched include PubMed, MEDLINE, and the Cochrane Library, utilizing key search terms such as "intestinal barrier function review," "metabolic endotoxemia," "claudin tight junctions," and "L-glutamine gut permeability." Evidence was graded in accordance with the GRADE framework.
¶ References
¶ Update Log
- 2026-07-07: Biological monograph created, detailing the tight junction complex, biochemical pathways of subclinical LPS translocation, sensitive biomarkers, and evidence-backed intestinal barrier repair protocols.
Mishra S, Jain S, Agadzi B. A Cascade of Microbiota-Leaky Gut-Inflammation- Is it a Key Player in Metabolic Disorders? Current obesity reports. 2025. https://pubmed.ncbi.nlm.nih.gov/40208464/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Basting CM, Schroeder TA, Ferbas KG. Gut barrier integrity biomarkers are associated with increased inflammation and predict disease status in hospitalized COVID-19 patients. Scientific reports. 2026. https://pubmed.ncbi.nlm.nih.gov/42399316/ ↩︎ ↩︎ ↩︎
Lee S. Systemic histopathological responses to nanoplastic exposure: A review of cellular toxicity and organ-level pathology in mammalian systems. Toxicology mechanisms and methods. 2026. https://pubmed.ncbi.nlm.nih.gov/42402713/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Matar A, Abdelnaem N, Camilleri M. Bone Broth Benefits: How Its Nutrients Fortify Gut Barrier in Health and Disease. Digestive diseases and sciences. 2025. https://pubmed.ncbi.nlm.nih.gov/40180691/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Camilleri M. Review: Human Intestinal Barrier-Optimal Measurement and Effects of Diet in the Absence of Overt Inflammation or Ulceration. Alimentary pharmacology & therapeutics. 2025. https://pubmed.ncbi.nlm.nih.gov/40515459/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Wang J, He Y, Liu Z. Glutamine Peptides: Preparation, Analysis, Applications, and Their Role in Intestinal Barrier Protection. Nutrients. 2025. https://pubmed.ncbi.nlm.nih.gov/40290078/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Abbasi F, Haghighat Lari MM, Khosravi GR. A systematic review and meta-analysis of clinical trials on the effects of glutamine supplementation on gut permeability in adults. Amino acids. 2024. https://pubmed.ncbi.nlm.nih.gov/39397201/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Khasanov R, Boettcher M, Wessel LM. All roads lead to NF-κB: the NF-κB pathway as a major target for intestinal inflammatory disorders. Frontiers in immunology. 2026. https://pubmed.ncbi.nlm.nih.gov/42148126/ ↩︎ ↩︎ ↩︎
Rosali MI, V Thanga Velu DP, Mokhtar MH. Specificity vs. Synergy Between Single-Strain and Multi-Strain Probiotics for Ulcerative Colitis Treatment: A Review of the Literature. Biomedicines. 2026. https://pubmed.ncbi.nlm.nih.gov/42351814/ ↩︎ ↩︎ ↩︎ ↩︎
Yin Z, Gong G, Yin J. Bidirectional communication between spinal cord injury and gut microbiota, from the bench to the bedside. Frontiers in immunology. 2026. https://pubmed.ncbi.nlm.nih.gov/42404902/ ↩︎
Li F, Wang Z, Cao Y. Intestinal Mucosal Immune Barrier: A Powerful Firewall Against Severe Acute Pancreatitis-Associated Acute Lung Injury via the Gut-Lung Axis. Journal of inflammation research. 2024. https://pubmed.ncbi.nlm.nih.gov/38617383/ ↩︎
Beyoğlu D, Idle JR. The Gut-Lung Microbiome Crosstalk and Pulmonary Disease. Biomolecules. 2026. https://pubmed.ncbi.nlm.nih.gov/42352300/ ↩︎
Sen BK, Pan K, Chakravarty A. Hepatic Encephalopathy: Current Thoughts on Pathophysiology and Management. Current neurology and neuroscience reports. 2025. https://pubmed.ncbi.nlm.nih.gov/40153081/ ↩︎