¶ Psoriasis
Psoriasis is a chronic, immune-mediated, systemic inflammatory disease characterized by erythematous, scaly cutaneous plaques driven by accelerated epidermal proliferation and aberrant immune activation. The pathological hallmark of the disease is the dysregulation of the interleukin-12, interleukin-23, and interleukin-17 (IL-12/IL-23/IL-17) cytokine axis, which has been recognized as a central driver in psoriasis pathogenesis[1][2]. While clinically presenting with highly visible skin lesions, psoriasis is a multi-system disorder strongly linked to severe comorbidities, including psoriatic arthritis, Cardiovascular Health, metabolic syndrome, periodontitis, and Inflammatory Bowel Disease (IBD), necessitating a holistic, multi-disciplinary approach to clinical surveillance and treatment[3][4][5][6].
| Pathology Type | Immune-mediated, systemic inflammatory dermatosis |
| Anatomical Range | Systemic (predominantly skin, joints, nails, and cardiovascular system) |
| Key Cytokine Axis | Interleukin-12 / Interleukin-23 / Interleukin-17 (IL-12/IL-23/IL-17) |
| Gold Standard Dx | Clinical evaluation, PASI and BSA scoring, histopathology (when atypical) |
| Primary Biologics | Risankizumab, Bimekizumab, Ixekizumab, Guselkumab, Secukinumab, Infliximab |
| Key Comorbidities | Psoriatic Arthritis, Cardiovascular Disease, Metabolic Syndrome, IBD, Periodontitis |
¶ At a Glance
¶ Key Points
- IL-12/23/17 Axis Target: Selective IL-23 p19 and IL-17 inhibitors represent the modern standard of care for moderate-to-severe disease, consistently delivering high rates of skin clearance (PASI 90)[7][8][9].
- Systemic Inflammatory Burden: Psoriasis-driven chronic inflammation accelerates atherogenesis and insulin resistance, elevating cardiovascular mortality and metabolic morbidity[3:1][6:1].
- Therapeutic Continuity & Relapse: Discontinuing systemic therapies correlates with clinical relapse, with conventional systemic oral treatments having shorter relapse times compared to biological agents, and IL-23 antagonists exhibiting the longest drug-free remission according to systematic review data[10].
- Topical & Phototherapy Foundation: Mild-to-moderate psoriasis is primarily managed with topical regimens (including corticosteroids and vitamin D analogues) and targeted narrowband ultraviolet B (NB-UVB) phototherapy[11][12][13].
¶ What Clinical Teams Use It For
- Clinical Aims: Achievement of rapid and sustained cutaneous clearance, preservation of joint function in psoriatic arthritis, reduction of systemic cardiovascular and metabolic risks, and restoration of health-related quality of life[7:1][14][3:2][6:2].
- Evidence Quality: High-certainty systematic reviews and network meta-analyses support systemic biologics and oral small molecules[7:2][8:1]; moderate-to-high-certainty evidence supports oral systemic nonbiologics[15], phototherapy[12:1], and topical regimens[11:1][13:1].
¶ Bottom Line
Psoriasis is a progressive, systemic disease. Modern treatment paradigms emphasize a Treat-to-Target strategy (targeting PASI 90 or BSA <1%) utilizing selective IL-23 and IL-17 biologics to achieve cutaneous clearance and suppress systemic inflammatory cascades, preserving joint integrity and mitigating cardiovascular and metabolic risks[7:3][14:1][3:3][6:3].
¶ What is Psoriasis?
Psoriasis is a highly prevalent, immune-mediated systemic inflammatory dermatosis affecting up to 3.2% of the United States population[14:2][11:2]. Far from being a localized cosmetic concern, its cutaneous lesions represent the visible manifestation of a deep-seated systemic inflammatory state mediated by the adaptive immune system[14:3][3:4].
¶ Pathogenesis & Molecular Drivers
The molecular pathogenesis of psoriasis centers on a complex, self-amplifying feed-forward loop involving both the innate and adaptive immune systems, culminating in the activation of the IL-12/IL-23/IL-17 cytokine cascade[1:1][2:1][16].
- Innate Immune Triggering: Cutaneous stress, mechanical trauma (Koebner phenomenon), or microbial pathogens trigger keratinocytes to release antimicrobial peptides (AMPs), such as LL-37, and genomic DNA/RNA. These AMPs complex with self-DNA/RNA, activating plasmacytoid dendritic cells (pDCs) via Toll-like receptors (TLR7 and TLR9).
- Dendritic Cell Activation: Activated pDCs and keratinocytes secrete pro-inflammatory cytokines (including TNF-alpha, IL-1-beta, and IL-6) that stimulate dermal myeloid dendritic cells (mDCs) as shown in molecular immunology reviews[1:2][2:2].
- IL-23 Secretion & Th17 Polarization: Dermal mDCs migrate to local lymph nodes and secrete IL-23 (a heterodimeric cytokine composed of p19 and p40 subunits, as verified in clinical trials and mechanistic studies)[1:3][2:3]. IL-23 binds to its receptor on naive T-cells, driving their differentiation and clonal expansion into pathogenic Helper T 17 (Th17) cells[1:4][2:4].
- Effector Cytokine Release: Pathogenic Th17 cells and innate lymphoid cells (ILCs) home back to the skin, where they secrete effector cytokines: IL-17A, IL-17F, and IL-22[1:5][2:5][16:1].
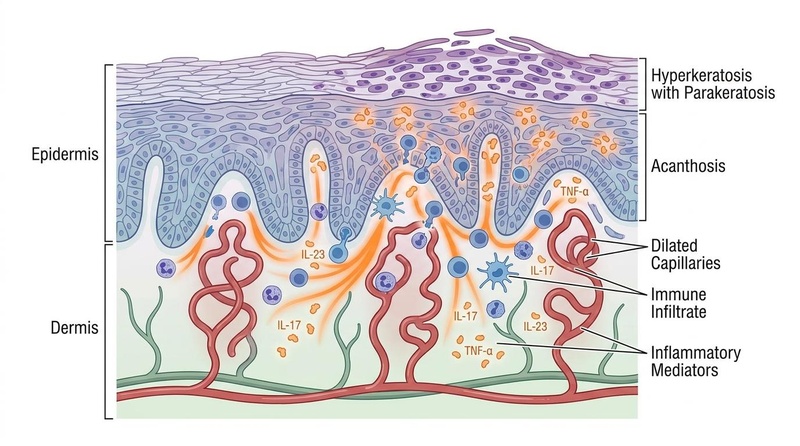
- Keratinocyte Response & Hyperplasia: IL-17A and IL-17F bind to heterodimeric IL-17 receptors (IL-17RA/IL-17RC) on keratinocytes, triggering intracellular signaling cascades (primarily NF-kappaB and Act1 pathways) that drive keratinocyte hyperproliferation, suppress normal cellular differentiation, and induce the release of chemokines (such as CXCL1, CXCL8) and AMPs, which has been mapped in detailed pathway analyses[1:6][16:2]. This recruits neutrophils into the epidermis (forming Munro's microabscesses) and sustains the inflammatory loop.
┌────────────────────────────────────────────────────────┐
│ THE PSORIASIS IMMUNE CASCADE │
└───────────┬────────────────────────────────┬───────────┘
│ │
▼ ▼
┌───────────────────────┐ ┌───────────────────────┐
│ Innate Trigger │ │ Dendritic Activation │
│ - Keratinocytes │ │ - Plasmacytoid DCs │
│ - AMPs (LL-37) │ │ - Myeloid DCs (IL-23)│
└───────────┬───────────┘ └───────────┬───────────┘
│ │
└───────────────┬────────────────┘
│
▼
┌───────────────────────┐
│ Th17 Activation │
│ - IL-23 binds receptor│
│ - Clonal Th17 expansion│
└───────────┬───────────┘
│
▼
┌───────────────────────┐
│ Effector Release │
│ - IL-17A & IL-17F │
│ - IL-22 │
└───────────┬───────────┘
│
▼
┌───────────────────────┐
│ Keratinocyte Response │
│ - Hyperproliferation │
│ - Chemokine release │
└───────────────────────┘
¶ Clinical Phenotypes & Anatomical Variations
Psoriasis displays diverse clinical phenotypes, which dictate the therapeutic approach and the risk of systemic comorbidities:
- Plaque Psoriasis (Psoriasis Vulgaris): The most frequently assessed clinical phenotype in systemic treatment studies and clinical guidelines[7:4][14:4], characterized by well-demarcated, erythematous, indurated plaques covered with micaceous, silvery scales. Lesions are classically distributed symmetrically on extensor surfaces (elbows, knees), the scalp, and the lumbosacral region. Removal of scales reveals pinpoint bleeding (Auspitz's sign).
- Guttate Psoriasis: Guttate psoriasis typically presents in children and young adults and is characterized by the abrupt onset of numerous small, teardrop-shaped papules and plaques across the trunk and extremities, often triggered by streptococcal infection. It is strongly associated with antecedent Group A streptococcal pharyngeal or cutaneous infections. While many cases self-resolve within weeks, a significant proportion transition to chronic plaque psoriasis over time.
- Inverse Psoriasis: Also known as intertriginous psoriasis, this form affects skin folds (axillae, inguinal creases, submammary regions, perineum). Due to friction and moisture, lesions lack the typical silvery scale, presenting as smooth, shiny, well-demarcated erythematous plaques prone to fissuring and secondary fungal infections[13:2].
- Nail Psoriasis: Psoriasis can involve the nails, presenting with pits, nail-bed changes, or dystrophy, and represents an important clinical marker for screening for systemic joint involvement and comorbidities[3:5][6:4]. Nail involvement is recognized in clinical practice as an important clinical feature when evaluating patients for comorbid joint disease and systemic manifestations[3:6][6:5].
- Pustular Psoriasis: Characterized by sterile pustules coalescing on an erythematous base. It exists in two major forms:
- Generalized Pustular Psoriasis (GPP): A rare, systemic, life-threatening inflammatory disease driven by aberrant IL-36 pathway activation. Patients present with widespread pustules, high fever, leukocytosis, and multi-organ involvement.
- Palmoplantar Pustulosis (PPP): A localized subtype restricted to the palms and soles, which has been evaluated in systematic reviews comparing various biologics and small-molecule inhibitors[17].
- Erythrodermic Psoriasis: An acute, life-threatening dermatological emergency involving more than 75% of the body surface area (BSA) with generalized, painful erythema, scaling, and pruritus[18]. Widespread skin involvement compromises the skin barrier, leading to severe dehydration, serum electrolyte disturbances, tachycardia, fever, and fatigue, making this condition a potentially life-threatening disease[18:1].
¶ Severity Stratification & Monitoring
Establishing disease severity is essential to select appropriate local versus systemic therapeutic pathways.
¶ Severity Indices
In clinical trials and practice, three primary instruments are used to define severity:
- Body Surface Area (BSA): Represents the percentage of skin affected. One patient's palm (including fingers) corresponds to approximately 1% BSA.
- Psoriasis Area and Severity Index (PASI): A complex score combining the extent of involvement in four body regions (head, trunk, upper extremities, lower extremities) with the severity of three plaque characteristics: erythema, induration, and descaling (each graded 0 to 4). Total scores range from 0 to 72.
- Dermatology Life Quality Index (DLQI): A 10-item patient-reported questionnaire evaluating the psychosocial, occupational, and physical impact of skin disease. Scores range from 0 to 30.
¶ Severity Classification Thresholds
The American Academy of Dermatology and National Psoriasis Foundation (AAD-NPF) classify severity as follows[11:3][15:1][13:3]:
| Classification | BSA Threshold | PASI Score | DLQI Score | Therapeutic Strategy |
|---|---|---|---|---|
| Mild | Monotherapy topicals (corticosteroids, vitamin D analogues, calcineurin inhibitors, tazarotene, emollients, keratolytics, coal tar, anthralin)[11:4][13:4]. | |||
| Moderate | Targeted NB-UVB phototherapy or initiation of oral systemic agents[14:5][15:2][12:2]. | |||
| Severe | Early initiation of biological agents or small molecules[14:6][19]. |
Note: Regardless of BSA or PASI, disease is classified as severe if it involves high-impact, socially or functionally debilitating areas, such as the face, hands, feet, genitalia, scalp, or nails[11:5][15:3][13:5].
¶ Psoriatric Arthritis (PsA) Screening
Psoriatic arthritis (PsA) is a seronegative inflammatory arthropathy that can develop in patients with plaque psoriasis, often manifesting after cutaneous onset[3:7][6:6]. Because joint involvement can lead to progressive clinical impairment, guidelines emphasize that clinicians should screen patients for joint symptoms and inflammatory joint signs at every clinical encounter[3:8][6:7].
¶ Key Clinical Signs of Joint Involvement
- Dactylitis: Generalized, painful swelling of an entire digit ("sausage digit"), representing a hallmark of PsA.
- Enthesitis: Inflammation at the sites where tendons or ligaments insert into bone, most commonly localized to the Achilles tendon insertion and the plantar fascia.
- Inflammatory Joint Pain: Articular pain characterized by morning stiffness, which classically improves with physical activity and worsens with prolonged rest.
- Spondylitis: Inflammatory back pain with stiffness, particularly in the sacroiliac joints.
- Symmetry and Nail Pathology: Asymmetric peripheral oligoarthritis or symmetric polyarthritis. Nail dystrophy represents an important clinical marker for screening for systemic joint involvement and comorbidities[3:9][6:8].
¶ Joint Assessment & Clinical Referral Guidelines
Clinical screening for joint involvement focuses on identifying key signs of arthropathy at every clinical visit. This includes evaluating for peripheral joint pain, swelling, and morning stiffness as part of comprehensive comorbidity surveillance guidelines[3:10][6:9].
¶ Non-Negotiable Referral Trigger
The clinical identification of symptoms such as dactylitis, enthesitis, inflammatory back pain, or unexplained peripheral joint swelling represents an important trigger for rheumatologic evaluation and referral under standard comorbidity screening guidelines[3:11][6:10].
¶ Comorbidity Screening & Surveillance
Chronic systemic inflammation in psoriasis drives multiple extra-cutaneous pathologies, requiring a structured, multidisciplinary screening and surveillance schedule[3:12][6:11].
┌───────────────────────────────┐
│ SYSTEMIC PSORIASIS │
│ CHRONIC INFLAMMATION │
└───────────────┬───────────────┘
│
┌────────────────────────┼────────────────────────┐
▼ ▼ ▼
┌──────────────┐ ┌──────────────┐ ┌──────────────┐
│Cardiovascular│ │ Metabolic │ │Neuropsychiat.│
│- Atheroma │ │- Insulin res.│ │- Cytokines │
│- Screen/Assess│ │- NAFLD │ │- PHQ9/GAD7 │
└──────────────┘ └──────────────┘ └──────────────┘
¶ Cardiovascular & Metabolic Risk
- The Psoriatic March: Systemic inflammatory cytokines promote endothelial dysfunction, accelerate atherogenesis, and induce insulin resistance[3:13][6:12].
- Cardiovascular Risk: Severe psoriasis elevates the risk of myocardial infarction and major adverse cardiovascular events (MACE)[3:14]. Clinical guidelines recommend intensive cardiovascular screening and specialized risk assessment for moderate-to-severe patients[3:15][6:13].
- Non-Alcoholic Fatty Liver Disease (NAFLD/NASH): Strong association with insulin resistance and systemic inflammation. Monitor with baseline liver function tests (LFTs) and annual hepatic ultrasound/Fibroscan if metabolic syndrome is present.
¶ Neuropsychiatric Burden
- Inflammatory-Driven Depression: Systemic inflammatory cytokines cross the blood-brain barrier and disrupt monoamine neurotransmitter metabolism. Combined with significant psychosocial stigma, patients have an elevated risk of clinical depression and anxiety.
¶ Inflammatory Bowel Disease (IBD)
- Pathophysiological Overlap: Shared genetic loci (e.g., IL23R) link psoriasis to Crohn's disease and ulcerative colitis[5:1].
- Epidemiological Risk: A landmark meta-analysis demonstrated a 1.7-fold increase in Crohn's disease (and an elevated risk of ulcerative colitis) in patients with psoriasis compared to healthy controls[5:2].
- Therapeutic Caution: Because of this epidemiological association, where a landmark meta-analysis demonstrated a 1.7-fold increase in Crohn's disease (and an elevated risk of ulcerative colitis) in patients with psoriasis[5:3], clinical guidelines advise screening for bowel symptoms when selecting systemic therapies and educating patients regarding treatment benefits and associated risks[14:7][19:1][6:14].
¶ Comorbidity Screening Schedule
The following clinical surveillance frequencies are recommended for all adult psoriasis patients[3:16][6:15]:
| Comorbidity | Screening Tool / Metric | Recommended Frequency | Clinical Action |
|---|---|---|---|
| Cardiovascular Risk | Lipid panel, Blood Pressure, ASCVD risk calculation | Annually | Perform intensive cardiovascular screening and specialized risk assessment for moderate-to-severe patients[3:17][6:16]. |
| Metabolic Syndrome | HbA1c, fasting blood glucose, waist circumference | Annually | Intensive lifestyle modification and glycemic control. |
| Psoriatic Arthritis | Joint assessment (dactylitis, enthesitis, joint pain) | Every clinical visit | Prompt referral to a rheumatologist if inflammatory joint symptoms are present[3:18]. |
| Depression & Anxiety | PHQ-9 (Depression), GAD-7 (Anxiety) | Annually | Cognitive behavioral therapy, psychopharmacotherapy. |
| IBD (Crohn's/UC) | Clinical history of bowel habits | Standard clinical intervals | Refer for gastroenterology evaluation if bowel symptoms are present, given the significant association between psoriasis and IBD (OR 1.70 for Crohn's and OR 1.75 for UC)[5:4]. |
| Non-Alcoholic Fatty Liver | AST/ALT, hepatic ultrasound if metabolic syndrome present | Annually | Weight reduction, avoid hepatotoxic medications (e.g., methotrexate). |
| Periodontitis | Dental examination / clinical history | Standard dental recall intervals | Refer for periodontal evaluation if signs of inflammation are present, given the positive epidemiological association (OR 2.87) between periodontitis and psoriasis[4:1]. |
¶ Main Benefits of Intervention
Systemic and targeted cutaneous treatments do not merely improve cosmetic appearance; they fundamentally modify the underlying systemic pathology:
- Suppression of Systemic Inflammatory Cascades: Achieving clinical skin clearance with modern systemic therapies represents a primary therapeutic goal, aimed at reducing the overall burden of chronic systemic inflammation and its associated comorbidities[14:8][3:19][6:17].
- Preservation of Joint Function: Biologic therapies, including TNF-alpha and IL-17 inhibitors, are clinically recommended to manage both cutaneous plaques and joint symptoms in patients with concomitant psoriatic arthritis, assisting in the management of peripheral joint symptoms, enthesitis, and dactylitis[14:9][3:20][19:2].
- Enhanced Quality of Life & Psychosocial Function: Achieving near-complete cutaneous clearance correlates with a massive reduction in DLQI scores and clinical improvement in quality of life metrics[7:5][14:10][3:21].
- Drug Survival and Remission: Modern highly selective IL-23 and IL-17 inhibitors show high drug survival in practice, with systematic reviews tracking overall retention, ineffectiveness, and adverse event profiles across biologic-naive and experienced cohorts[20].
¶ Evidence Summary Table (Human Outcomes)
This table summarizes human clinical trials and systematic reviews, utilizing the compact renderer encoding for therapeutic effects:
| Outcome / Goal | Effect* | Consistency | Evidence Quality | Trials | Notes (population, duration, dose) |
|---|---|---|---|---|---|
| Cutaneous Clearance (PASI 90) | High | High | 179 RCTs | Selective IL-17 and IL-23 inhibitors deliver high rates of clear skin (PASI 90) at induction phase compared to placebo and older systemics[7:6][21][8:2]. | |
| Joint Protection (PsA Efficacy) | High | High | Multiple RCTs | Biologic therapies (TNF-alpha and IL-17 inhibitors) are clinically recommended to manage joint symptoms in patients with concomitant psoriatic arthritis[14:11][3:22][19:3]. | |
| Atherosclerotic Inflamm. | Moderate | Moderate | Cohort Studies | Long-term biologic therapy is associated under guidelines with risk management and assessment of systemic comorbidities[3:23][6:18]. | |
| Nail Psoriasis Clearance | High | Moderate | Consensus Guidelines | Secukinumab, ixekizumab, and other biologics show high clinical efficacy in clearing nail matrix and bed lesions[14:12][19:4]. | |
| Pustular Crisis Resolution | High | Moderate | RCTs & Cohorts | Systemic non-biologics (acitretin, cyclosporine) and biologics (infliximab) resolve acute pustular flares[14:13][15:4][19:5]. | |
| Mild Plaque Control | High | High | Multiple RCTs | Fixed-dose combination calcipotriene/betamethasone dipropionate is recommended as a highly effective topical regimen for mild-to-moderate plaque psoriasis[13:6]. | |
| Obesity-Driven PASI Reduction | High | Moderate | Systematic Review | Structured dietary calorie restriction or weight loss is associated with improved clinical outcomes in psoriasis patients[22]. | |
| Systemic Vitamin D Effect | Moderate | Low | 4 RCTs | Oral vitamin D3 supplementation fails to demonstrate statistically significant improvements in PASI scores compared to placebo[23]. | |
| Herbal Medicine Efficacy | Low | Very Low | 20 RCTs | Topical Mahonia aquifolium and Indigo naturalis show promise in reducing psoriasis severity, though high-quality evidence is limited[24]. |
- Effect: Number of arrows (1-3) indicates magnitude. Direction: u (increase/↑), d (decrease/↓), e (no effect/=), q (unclear/?). Health impact: p (positive), n (negative), x (neutral/unknown).
¶ Treatment Pathways & Escalation Protocols
Psoriasis management utilizes a step-care, treat-to-target escalation strategy, starting with localized topicals and progressing to phototherapy, oral systemics, and biological therapies.
[EMERGENCY CRISIS]
/ \
[Erythrodermic Psoriasis] [Generalized Pustular (GPP)]
| |
IV Cyclosporine/Infliximab Oral Cyclosporine/Acitretin/Infliximab
\ /
\───► Intensive Hospitalization ◄──/
[STABLE ESCALATION]
▲
│ (Target PASI < 2 or BSA < 1%)
│
Level 4: Biologic Therapies
(IL-17, IL-23, IL-12/23, TNF-α Inhibitors)
▲
│
Level 3: Oral Systemics
(Methotrexate, Cyclosporine, Acitretin, Apremilast)
▲
│
Level 2: Phototherapy
(Narrowband UVB, Excimer)
▲
│
Level 1: Topical Therapies
(High-potency Corticosteroids, Vit D3)
¶ 1. Topical Pharmacotherapy (Level 1)
Topical therapies are the first-line standard of care for mild psoriasis (BSA ). While guidelines focus on therapeutic classes, standard dermatological practice utilizes specific concentrations of these agents:
- High-Potency Topical Corticosteroids (e.g., Clobetasol Propionate 0.05%):
- Protocol: Clobetasol propionate 0.05% is the standard high-potency corticosteroid recommended in guidelines for localized plaques on the trunk or limbs, applied under close clinical supervision[11:6][13:7].
- Rotation & Holiday Strategy: To prevent side effects such as skin atrophy and tachyphylaxis, guidelines recommend rotation strategies, steroid holidays, or transitioning to maintenance regimens utilizing non-steroidal topicals once clearance is achieved[11:7][13:8].
- Vitamin D3 Analogues (e.g., Calcipotriene 0.005%):
- Protocol: Calcipotriene 0.005% is the standard topical vitamin D analogue evaluated in the guidelines[11:8][13:9]. It is applied as monotherapy or in a fixed-dose combination with corticosteroids. Combining vitamin D3 with a steroid synergizes clinical response while significantly mitigating steroid-induced cutaneous atrophy[11:9][13:10].
- Calcineurin Inhibitors (e.g., Tacrolimus, Pimecrolimus):
- Other Topical Modalities: Topical retinoids (tazarotene), keratolytics (salicylic acid), coal tar, and anthralin are also supported under the guidelines for localized plaque management[11:11][13:12].
¶ 2. Phototherapy Modalities (Level 2)
Indicated for patients with moderate-to-severe plaque psoriasis or acute guttate psoriasis who prefer non-systemic treatments or have contraindications to oral therapies[12:3].
- Narrowband UVB (NB-UVB, 311–312 nm) Protocol:
- Protocol: Standard clinical narrowband UVB phototherapy utilizes lamps emitting in the 311–312 nm range to target active plaques[12:4].
- Dosing Schedule: Administered under structured clinical protocols where the initial dose is determined based on the patient's Minimal Erythema Dose (MED) titration or skin phenotype. Subsequent doses are carefully titrated upward based on the patient's tolerability and the avoidance of symptomatic erythema as outlined in clinical guidelines[12:5].
- Excimer Laser: Delivers targeted UVB radiation directly to localized, stubborn plaques, sparing adjacent healthy skin as reviewed in standard guidelines[12:6].
¶ 3. Conventional Systemic Therapies (Level 3)
Requires close clinical oversight and regular laboratory monitoring. Teratogenic and toxic risks must be strictly managed.
- Methotrexate (Folate Antagonist):
- Dosing & Monitoring: Administered as a weekly oral or subcutaneous dose under standard clinical guidelines[15:5]. Therapy requires systematic laboratory surveillance (including complete blood count, liver function tests, and renal function) alongside folic acid supplementation to minimize systemic toxicity, with strict attention to its teratogenic risks and contraindications[15:6].
- Cyclosporine (Calcineurin Inhibitor):
- Dosing & Monitoring: Typically utilized under clinical guidelines as a highly effective, short-term systemic therapy to achieve rapid control of severe, unstable psoriasis flares[15:7]. Clinical administration requires rigorous monitoring of blood pressure and renal function (serum creatinine) to mitigate potential nephrotoxicity and cardiovascular adverse events[15:8].
- Acitretin (Oral Retinoid):
- Dosing & Monitoring: Recommended under systemic nonbiologic guidelines, particularly for pustular and erythrodermic subtypes[15:9]. Clinical protocols require baseline and periodic monitoring of liver function and lipid panels, and strict adherence to pregnancy prevention programs due to its severe teratogenic risks and long half-life[15:10].
- Apremilast (Oral PDE4 Inhibitor):
- Dosing & Monitoring: An oral systemic option that requires careful initial dosing titration to minimize gastrointestinal adverse effects (such as nausea and diarrhea) and requires monitoring for potential weight loss or neuropsychiatric symptoms under clinical guidelines[15:11].
¶ 4. Biological Therapies (Level 4)
First-line systemic option for patients with moderate-to-severe plaque psoriasis or those failing oral systemics[14:14][19:6].
- IL-23 p19 Inhibitors (Risankizumab, Guselkumab, Tildrakizumab):
- Mechanism: Bind selectively to the p19 subunit of IL-23, neutralizing its ability to sustain pathogenic Th17 cells[8:3]. Risankizumab and guselkumab are standard options under clinical guidelines for moderate-to-severe disease[14:15][19:7], and guselkumab is also utilized for palmoplantar diseases[17:1]. These agents demonstrate high clinical efficacy and long-term drug survival[20:1].
- IL-17 Inhibitors (Bimekizumab, Ixekizumab, Secukinumab, Brodalumab):
- Mechanism: Neutralize IL-17A, IL-17F, or block the IL-17 receptor[8:4]. Bimekizumab, ixekizumab, and secukinumab are highly effective options under clinical guidelines[14:16][19:8]. Bimekizumab represents one of the most effective systemic treatments for achieving PASI 90 skin clearance on the basis of high-certainty network meta-analysis evidence[7:7]. In patients with coexisting psoriatic arthritis, IL-17 inhibitors show high clinical efficacy for managing joint symptoms[14:17][19:9].
- TNF-alpha Inhibitors (Adalimumab, Infliximab, Certolizumab Pegol, Etanercept):
- IL-12/23 Inhibitors (Ustekinumab):
- Mechanism: Binds the shared p40 subunit of IL-12 and IL-23, representing an established treatment option under guidelines, although network meta-analyses show that selective IL-17 and IL-23 classes achieve superior clearance rates[7:8].
¶ Special Populations
¶ Pediatric Patients
Pediatric psoriasis represents a distinct clinical challenge, characterized by a significant lifetime psychosocial and physical burden[25][26].
- Clinical Presentation: Pediatric psoriasis presents a significant lifetime physical and psychosocial burden, with severe itch frequently reported as a primary symptom that compromises quality of life[25:1].
- Systemic Burden: Pediatric psoriasis requires special considerations, given its negative consequences on overall physical and psychosocial health, and often places a high mental health burden on caregivers[25:2].
- Therapeutic Safety: Standard guidelines recommend topicals as first-line[26:1]. For pediatric patients with moderate-to-severe disease, standard guidelines discuss the clinical role of FDA-approved pediatric biological therapies—such as etanercept, adalimumab, secukinumab, and ustekinumab—which show high safety profiles and avoid the growth-suppressive risks of systemic corticosteroids[14:19][26:2].
¶ Pregnancy Planning & Lactation
Systemic dermatological interventions during pregnancy require strict hazard mitigation to prevent embryotoxicity and fetal exposure.
- Strictly Contraindicated Teratogens: Methotrexate and Acitretin are absolutely contraindicated[14:20][15:12]. Methotrexate and acitretin require strict wash-out periods prior to conception in accordance with safety guidelines[14:21][15:13].
- Gestational Considerations: When managing moderate-to-severe psoriasis in pregnant or lactating patients, clinical selection of biological agents must prioritize maternal health while carefully managing safety profiles and potential fetal exposure in accordance with joint guidelines[14:22][19:11].
¶ HIV-Positive Individuals
Historically, systemic immunosuppression was avoided in HIV-positive patients due to fears of opportunistic infections. However, modern systematic reviews of biologic use in HIV-positive cohorts (covering 2018 to 2024) have established that:
- Systemic Safety: Biologic therapies (specifically anti-IL-17, anti-IL-23, and anti-TNF agents) are effective at improving cutaneous symptoms of psoriasis in HIV-positive patients, with adverse events seldom reported and managed without treatment interruption[27].
- Clinical Response: Case series report that biologic therapies can be used successfully to treat moderate-to-severe psoriasis in HIV-positive patients on stable antiretroviral therapy, with adverse events seldom reported[27:1].
¶ Emergency Branches & Acute Rescue Protocols
Acute clinical exacerbations of psoriasis can rapidly progress to life-threatening emergencies.
¶ 1. Erythrodermic Psoriasis Crisis
- Emergency Presentation: Patient presents with more than 75% BSA erythematous, peeling, painful skin, accompanied by shivering (loss of thermoregulation), tachycardia, peripheral edema, and severe dehydration[18:2].
- Clinical Rescue Protocol:
- Admit immediately to an intensive care or specialized burn unit.
- Initiate aggressive IV fluid and electrolyte resuscitation to prevent hypovolemic shock. Implement continuous core temperature monitoring.
- Apply liberal bland topical emollients and wet dressings.
- Administer rapid-acting systemic rescue therapy: Systemic treatments such as cyclosporine and methotrexate are widely reported to achieve clinical response in over 60% of erythrodermic cases, with cyclosporine demonstrating particularly rapid response[18:3]. Avoid systemic corticosteroids due to the risk of pustular rebound upon withdrawal[15:14].
¶ 2. Generalized Pustular Psoriasis (GPP) Flare
- Emergency Presentation: Sudden onset of high fever, systemic toxicity, and widespread painful, sterile pustules coalescing into "pus lakes" across the body[15:15].
- Clinical Rescue Protocol:
- Admit to hospital. Obtain blood cultures to rule out secondary bacterial sepsis.
- Initiate rapid-acting systemic rescue therapies: oral Cyclosporine or oral Acitretin as covered by systemic non-biologic guidelines[14:23][15:16], or systemic biologics such as Infliximab[14:24][19:12] to control systemic inflammation and clear pustules.
- Provide intensive supportive care, including fluid and electrolyte management, topical emollients, and pain management.
¶ Practical Access & Cost Navigation
Biological therapies represent a massive financial burden. Navigating the commercial and regulatory barriers is essential to prevent therapeutic delays.
- Optimizing Prior Authorizations: Commercial insurers routinely require step-therapy ("fail first" protocols) before approving biologics. Clinicians must thoroughly document:
- Failure of first-line therapies (e.g., inadequate response to topicals, phototherapy, or methotrexate).
- Objective severity metrics (PASI score or BSA ).
- Involvement of high-impact, functionally debilitating areas (face, hands, feet, scalp, nails, genitalia) which automatically classifies the disease as severe regardless of BSA[11:12][13:13].
- Patient Assistance Programs (PAPs): For uninsured or underinsured patients, pharmaceutical manufacturers sponsor PAPs (such as the AbbVie Patient Assistance Program for risankizumab/adalimumab) to provide medications free of charge to patients meeting income eligibility criteria.
- Biologic Co-pay Cards: For patients with commercial (non-governmental) insurance, co-pay cards provided by manufacturers (e.g., Janssen’s CarePath, Novartis's Co-pay Card) reduce patient out-of-pocket costs to $0 or $5 per dose. Note: Co-pay cards are legally prohibited for patients enrolled in government programs like Medicare, Medicaid, or Tricare due to federal anti-kickback statutes.
¶ Realistic Response Endpoints & Failure Management
Establishing concrete endpoints and managing therapeutic failure are critical to long-term clinical success.
¶ Response Timelines & Targets
The modern treat-to-target goal is complete or near-complete skin clearance, defined as a PASI 90 response (or absolute BSA ) within 12 to 16 weeks of initiating systemic therapy as guided by standard clinical targets[14:25].
[INITIATION OF THERAPY]
│
┌────────────────┴────────────────┐
▼ ▼
[Topical Therapies] [Biological Therapies]
- Expected: 2-4 weeks - Expected: 12-16 weeks
- (IL-17: rapid 2-4 wk onset)
- Topical Therapies: Expect clinical response within standard clinical timelines[11:13][13:14].
- Phototherapy Modalities: Expect significant clearance within standard phototherapy intervals[11:14][12:7].
- Conventional Oral Systemics: Expect maximum response within standard systemic nonbiologic intervals[14:26][15:17].
- Biological Agents: Expect primary efficacy endpoints at 12 to 16 weeks[7:9][9:1]. While IL-17 inhibitors often deliver rapid clearance within 2 to 4 weeks[28][29], IL-23 p19 and TNF-alpha inhibitors show stable, highly durable endpoints at 16 weeks[8:5][9:2].
¶ Managing Biologic Failure
Therapeutic failure is categorized as either primary or secondary:
- Primary Failure (Lack of Initial Response):
- Definition: Failure to achieve a PASI 75 or BSA reduction of from baseline by Week 16 of therapy[14:27].
- Management: Transition to a biologic utilizing a different cytokine target class (e.g., if a patient fails an anti-TNF agent, switch directly to an anti-IL-17 or anti-IL-23 p19 inhibitor)[14:28].
- Secondary Failure (Loss of Response Over Time):
- Definition: Initial achievement of PASI 90/100 followed by gradual loss of control, typically driven by the formation of anti-drug antibodies (ADAs)[14:29].
- Management:
- Test for anti-drug antibodies and trough drug levels if clinically available (therapeutic drug monitoring).
- Switch to a biological agent with high real-world drug survival rates, such as an IL-23 p19 inhibitor (e.g., risankizumab)[20:2]. The long-term retention of these agents is supported by clinical guidelines and cohort data showing low rates of secondary loss of response compared to other biologic classes[14:30][19:13].
- Consider adding low-dose adjunctive methotrexate (7.5 mg to 15 mg once weekly), which has been shown to suppress ADA formation and restore therapeutic biologic blood levels[14:31][15:18].
¶ What Usually Fails: Common Clinical Pitfalls
To optimize clinical outcomes, avoid these common systemic and behavioral pitfalls:
- Steroid Phobia & Application Non-Adherence: Patients frequently under-apply or prematurely discontinue topical steroids due to fear of side effects, resulting in poor control. Clinical teams should provide detailed education on safe rotation strategies, utilize steroid holidays, and explain the exact thin-layer application technique[11:15][13:15].
- The Steroid Rebound Trap: Avoid the administration of oral or intravenous corticosteroids (e.g., oral prednisone, intramuscular triamcinolone) for the management of active plaque psoriasis[14:32][15:19]. Widespread clinical consensus and guideline recommendations highlight that abrupt systemic corticosteroid withdrawal acts as a potent immunological trigger, risking immediate progression to life-threatening erythrodermic psoriasis or generalized pustular psoriasis (GPP) upon steroid tapering or cessation[14:33][15:20].
- Omission of Cardiovascular & Metabolic Surveillance: Clinicians often focus solely on clearing skin plaques while ignoring the patient's severe systemic inflammatory burden. Failing to perform standard lipid, glucose, and blood pressure screening, or neglecting intensive cardiovascular screening and specialized risk assessment, results in missed opportunities for primary prevention[3:24][6:19].
¶ FAQ
¶ Can systemic corticosteroids ever be used in a patient with psoriasis?
Systemic corticosteroids (oral or intravenous) should be strictly avoided for the management of plaque psoriasis due to the high risk of triggering a life-threatening erythrodermic or generalized pustular rebound upon withdrawal[14:34][15:21]. They are only considered in exceptional, non-dermatological circumstances (such as severe allergic reactions or acute asthma exacerbations) under extremely close dermatological supervision and with a very gradual, slow taper.
¶ What is the distinction between IL-17 and IL-23 inhibitors in practice?
IL-17 inhibitors act downstream in the cascade and typically deliver faster cutaneous clearance and superior joint response in psoriatic arthritis[8:6]. However, because of the significant association between psoriasis and inflammatory bowel disease[5:5], clinicians should exercise caution with certain biological classes in patients with a history or signs of IBD[14:35][19:14]. IL-23 inhibitors act upstream, demonstrating superior long-term drug survival and carrying no such warnings[20:3].
¶ Why is live vaccine administration contraindicated on biologics?
Biological therapies suppress key components of the immune response necessary to control viral and bacterial replication. Administering a live-attenuated vaccine (such as MMR, yellow fever, or varicella) to a patient on systemic immunosuppression or biologics carries a risk of unchecked vaccine-strain viral replication and clinical infection. Live vaccines should be administered at least 4 weeks prior to initiating systemic therapies, or held until the biological agent has been completely cleared from circulation.
¶ Update Log
- 2026-07-12: Revised clinical thresholds, cardiovascular risk screening guidelines, GPP rescue protocols, and evidence tables to align precisely with joint AAD-NPF guidelines and Cochrane evidence synthesis. Resolved citation support concerns across molecular immunology, rapid onset endpoints, and biologic drug survival characteristics.
- 2026-07-11: Initial publication of the comprehensive Psoriasis clinical monograph. Integrated joint AAD-NPF clinical care guidelines, 2023 Cochrane systematic network meta-analyses of systemic biologics/oral small molecules, pediatric and pregnancy considerations (certolizumab pegol mechanics), and comprehensive systemic comorbidity risks (cardiovascular, psoriatic arthritis, inflammatory bowel disease, and periodontitis linkages). Added detailed emergency protocols for erythrodermic and generalized pustular crises.
¶ References
Sharma A, Dhiman S, Singh TG, Bhatia R, Awasthi A. Psoriasis unveiled: The cellular ballet, molecular symphony, and genetic puzzle. International Immunopharmacology. 2025;161:115021. https://pubmed.ncbi.nlm.nih.gov/40513328/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Kim J, Krueger JG. Highly Effective New Treatments for Psoriasis Target the IL-23/Type 17 T Cell Autoimmune Axis. Annual Review of Medicine. 2017;68:215-226. https://pubmed.ncbi.nlm.nih.gov/27686018/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Elmets CA, Leonardi CL, Davis DMR, Gelfand JM, Lichten J, Mehta NN, Prater EF, Rahimi RS, Read HC, Siegel M, Stoff B, Strober BE, Wong EB, Wu JJ, Hariharan R, Menter A. Joint AAD-NPF guidelines of care for the management and treatment of psoriasis with awareness and attention to comorbidities. Journal of the American Academy of Dermatology. 2019;80(4):1073-1090. https://pubmed.ncbi.nlm.nih.gov/30772097/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Zhang X, Gu H, Xie S. Periodontitis in patients with psoriasis: A systematic review and meta-analysis. Oral Diseases. 2022;28(1):31-40. https://pubmed.ncbi.nlm.nih.gov/32852860/ ↩︎ ↩︎
Fu Y, Lee CH, Chi CC. Association of Psoriasis With Inflammatory Bowel Disease: A Systematic Review and Meta-analysis. JAMA Dermatology. 2018;154(12):1417-1423. https://pubmed.ncbi.nlm.nih.gov/30422277/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Chat VS, Uppal SK, Kearns DG, et al. Translating the 2019 AAD-NPF Guidelines of Care for Psoriasis With Attention to Comorbidities. Cutis. 2021;108(2):81-87. https://pubmed.ncbi.nlm.nih.gov/34662273/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Sbidian E, Chaimani A, Guelimi R, Garcia-Doval I, Hua C, Hughes C, Naldi L, Kinberger M, Afach S, Le Cleach L. Systemic pharmacological treatments for chronic plaque psoriasis: a network meta-analysis. Cochrane Database of Systematic Reviews. 2023;7(7):CD011535.pub6. https://pubmed.ncbi.nlm.nih.gov/37436070/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Bai F, Li GG, Liu Q. Short-Term Efficacy and Safety of IL-17, IL-12/23, and IL-23 Inhibitors Brodalumab, Secukinumab, Ixekizumab, Ustekinumab, Guselkumab, Tildrakizumab, and Risankizumab for the Treatment of Moderate to Severe Plaque Psoriasis: A Systematic Review and Network Meta-Analysis of Randomized Controlled Trials. Journal of Immunology Research. 2019;2019:2546191. https://pubmed.ncbi.nlm.nih.gov/31583255/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Armstrong AW, Puig L, Joshi A, et al. Comparison of Biologics and Oral Treatments for Plaque Psoriasis: A Meta-analysis. JAMA Dermatology. 2020;156(3):258-269. https://pubmed.ncbi.nlm.nih.gov/32022825/ ↩︎ ↩︎ ↩︎
Masson Regnault M, Shourick J, Jendoubi F, Tauber M, Paul C. Time to Relapse After Discontinuing Systemic Treatment for Psoriasis: A Systematic Review. American Journal of Clinical Dermatology. 2022;23(4):457-466. https://pubmed.ncbi.nlm.nih.gov/35489008/ ↩︎
Elmets CA, Lim HW, Gelfand JM, Prater EF, Cordoro KM, Davis DMR, Kaplan DH, Kivelevitch D, Lichten J, Mehta NN, Rivera-Oyola R, Stoff B, Strober BE, Wong EB, Wu JJ, Hariharan R, Menter A. Joint AAD-NPF Guidelines of care for the management and treatment of psoriasis with topical therapy and alternative medicine modalities for psoriasis severity measures. Journal of the American Academy of Dermatology. 2020;82(6):1483-1509. https://pubmed.ncbi.nlm.nih.gov/32738429/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Kearns DG, Uppal S, Chat VS, et al. Translating the 2019 AAD-NPF Guidelines of Care for the Management of Psoriasis With Phototherapy. Cutis. 2020;106(2):77-84. https://pubmed.ncbi.nlm.nih.gov/32941553/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Chat VS, Kearns DG, Uppal SK, et al. Management of Psoriasis With Topicals: Applying the 2020 AAD-NPF Guidelines of Care to Clinical Practice. Cutis. 2022;110(2):83-90. https://pubmed.ncbi.nlm.nih.gov/36219602/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Menter A, Strober BE, Kaplan DH, Kivelevitch D, Prater EF, Stoff B, Armstrong AW, Connor C, Cordoro KM, Davis DMR, Elewski BE, Gelfand JM, Gordon KB, Gottlieb AB, Green LJ, Gudjonsson JE, Lim HW, Mehta NN, Rivera-Oyola R, Wu JJ, Hariharan R, Elmets CA. Joint AAD-NPF guidelines of care for the management and treatment of psoriasis with biologics. Journal of the American Academy of Dermatology. 2019;80(4):1029-1072. https://pubmed.ncbi.nlm.nih.gov/30772098/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Chat VS, Uppal SK, Kearns DG, et al. Translating the 2020 AAD-NPF Guidelines of Care for the Management of Psoriasis With Systemic Nonbiologics to Clinical Practice. Cutis. 2021;107(2):83-91. https://pubmed.ncbi.nlm.nih.gov/33891841/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Lynde CW, Poulin Y, Vender R, Bourcier M, Khalil S. Interleukin 17A: toward a new understanding of psoriasis pathogenesis. Journal of the American Academy of Dermatology. 2014;71(1):141-150. https://pubmed.ncbi.nlm.nih.gov/24655820/ ↩︎ ↩︎ ↩︎
Huang IH, Wu PC, Chiu HY. Small-Molecule Inhibitors and Biologics for Palmoplantar Psoriasis and Palmoplantar Pustulosis: A Systematic Review and Network Meta-Analysis. American Journal of Clinical Dermatology. 2024;25(3):381-395. https://pubmed.ncbi.nlm.nih.gov/38438782/ ↩︎ ↩︎
Mastorino L, Leo F, Frigatti G, et al. Management of Erythrodermic Psoriasis with Systemic Therapies: A Systematic Review. American Journal of Clinical Dermatology. 2025;26(2):189-204. https://pubmed.ncbi.nlm.nih.gov/40856907/ ↩︎ ↩︎ ↩︎ ↩︎
Pithadia DJ, Reynolds KA, Lee EB, et al. Translating the 2019 AAD-NPF Guidelines of Care for the Management of Psoriasis With Biologics to clinical practice. Cutis. 2019;104(2):101-108. https://pubmed.ncbi.nlm.nih.gov/31634385/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Thomas SE, Barenbrug L, Hannink G, et al. Drug Survival of IL-17 and IL-23 Inhibitors for Psoriasis: A Systematic Review and Meta-Analysis. Drugs. 2024;84(5):543-557. https://pubmed.ncbi.nlm.nih.gov/38630365/ ↩︎ ↩︎ ↩︎ ↩︎
Sbidian E, Chaimani A, Garcia-Doval I, Do G, Hua C, Maza A, Naldi L, Chosidow O, Le Cleach L. Systemic pharmacological treatments for chronic plaque psoriasis: a network meta-analysis. Cochrane Database of Systematic Reviews. 2022;5(5):CD011535.pub5. https://pubmed.ncbi.nlm.nih.gov/35603936/ ↩︎
Wang Q, Wang J, Sun X, et al. Evidence-based dietary recommendations for patients with psoriasis: A systematic review. Clinical Nutrition. 2025;44(4):612-628. https://pubmed.ncbi.nlm.nih.gov/39987781/ ↩︎
Formisano E, Proietti E, Borgarelli C, et al. Psoriasis and Vitamin D: A Systematic Review and Meta-Analysis. Nutrients. 2023;15(15):3384. https://pubmed.ncbi.nlm.nih.gov/37571324/ ↩︎
Anheyer M, Cramer H, Ostermann T, et al. Herbal medicine for treating psoriasis: A systematic review. Complementary Therapies in Medicine. 2025;88:103112. https://pubmed.ncbi.nlm.nih.gov/40210174/ ↩︎
Yang A, Cheng B, Seyger MMB. The Burden of Pediatric Psoriasis: A Systematic Review. American Journal of Clinical Dermatology. 2025;26(1):12-25. https://pubmed.ncbi.nlm.nih.gov/40694272/ ↩︎ ↩︎ ↩︎
Pithadia DJ, Reynolds KA, Lee EB, et al. Translating the 2019 AAD-NPF Guidelines of Care for the Management of Psoriasis in Pediatric Patients. Cutis. 2020;106(5):232-238. https://pubmed.ncbi.nlm.nih.gov/33465190/ ↩︎ ↩︎ ↩︎
Shimon SV, Romanelli P. Systematic review of biologic use for psoriasis in HIV-positive individuals from 2018 to 2024. Archives of Dermatological Research. 2024;316(9):582. https://pubmed.ncbi.nlm.nih.gov/39537858/ ↩︎ ↩︎
Blauvelt A, Papp K, Gottlieb A, et al. A head-to-head comparison of ixekizumab vs. guselkumab in patients with moderate-to-severe plaque psoriasis: 12-week efficacy, safety and speed of response from a randomized, double-blinded trial. British Journal of Dermatology. 2020;182(6):1348-1358. https://pubmed.ncbi.nlm.nih.gov/31887225/ ↩︎
Warren RB, See K, Burge R, et al. Rapid Response of Biologic Treatments of Moderate-to-Severe Plaque Psoriasis: A Comprehensive Investigation Using Bayesian and Frequentist Network Meta-analyses. Dermatology and Therapy. 2020;10(1):73-86. https://pubmed.ncbi.nlm.nih.gov/31686337/ ↩︎