¶ Regulatory Landscape for Longevity Interventions: Pathways and Oversight
The regulatory landscape for longevity interventions is intricate and rapidly evolving, presenting unique challenges for researchers, clinicians, and individuals seeking to extend healthspan. Unlike traditional therapeutics that target specific diseases, many longevity approaches aim to modulate fundamental aging processes, which are not yet universally classified as diseases. This creates significant "gray areas" in approval pathways, oversight, and consumer access.
¶ Quick Answer
The regulatory environment for longevity interventions is highly complex, often operating in "gray areas" due to aging not being universally classified as a disease. While traditional FDA/EMA approval pathways exist for disease-specific treatments, many longevity interventions utilize off-label prescribing, compounding pharmacies, or fall into unregulated medical tourism. Navigating this landscape requires careful consideration of scientific evidence, safety, and legal compliance.
¶ What It Is: Navigating the Regulatory Maze
Longevity interventions encompass a broad range of pharmaceutical, biological, and lifestyle approaches designed to extend healthspan by targeting the fundamental mechanisms of aging. Regulating these interventions is challenging because the traditional medical framework focuses on treating specific diseases, whereas aging itself is a complex biological process not yet universally recognized as a disease state by regulatory bodies. This distinction profoundly impacts the approval process, oversight, and accessibility of anti-aging therapies.
¶ Traditional Regulatory Pathways: The Gold Standard
For longevity interventions seeking formal regulatory approval, traditional pathways through agencies like the FDA (U.S. Food and Drug Administration) and EMA (European Medicines Agency) remain the gold standard. These pathways ensure rigorous testing for safety, efficacy, and quality.
¶ FDA and EMA Approval Processes
Drug development in the U.S. typically begins with an Investigational New Drug (IND) application, allowing a substance to be tested in humans. Clinical trials then proceed through three phases:
- Phase I: Small studies (20-100 healthy volunteers) focusing on safety, dosage, and pharmacokinetics.
- Phase II: Larger studies (100-300 patients) evaluating efficacy and further assessing safety.
- Phase III: Large-scale studies (hundreds to thousands of patients) confirming efficacy, monitoring adverse reactions, and comparing with existing treatments.
- Upon successful completion of trials, a New Drug Application (NDA) or Biologics License Application (BLA) is submitted for market approval.
¶ Accelerated Approval, Expanded Access, Compassionate Use, and Right to Try
The FDA provides mechanisms for expedited access to promising drugs for serious or life-threatening conditions:
- Accelerated Approval: Allows earlier approval for drugs addressing unmet medical needs in serious conditions, based on surrogate endpoints likely to predict clinical benefit. Post-market studies are required to confirm benefits [1].
- Expanded Access (Compassionate Use): Provides pathways for patients with serious conditions to access investigational drugs outside of clinical trials when no other satisfactory options exist [2].
- Right to Try Act: A federal law allowing patients with life-threatening diseases who have exhausted approved treatments to access certain unapproved investigational drugs directly from manufacturers, with reduced FDA oversight [3][4]. This pathway is distinct from Expanded Access and has generated debate regarding patient safety [3:1].
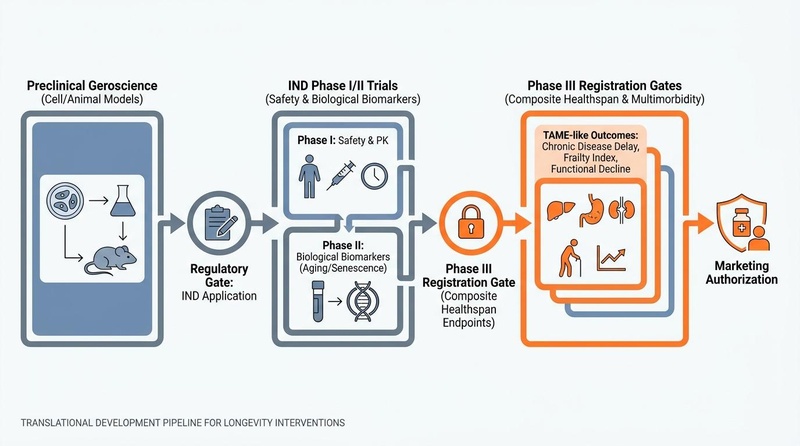
Figure 1: The translational pipeline and regulatory approval gates for longevity interventions, transitioning from disease-centric endpoints to systemic healthspan metrics.
¶ The Gray Market: Compounding and Off-Label Use
A significant portion of longevity interventions operates in a regulatory "gray market," characterized by off-label prescribing, specialized compounding, and direct-to-consumer (DTC) sales in less regulated environments.
¶ Off-Label Prescribing
Off-label prescribing occurs when a physician prescribes an FDA-approved drug for an indication, dosage, or patient population not specified in the drug's official labeling. While legal and often medically appropriate, it places a greater burden of responsibility on the prescribing clinician for patient safety and efficacy. For longevity interventions, off-label use is common for drugs like metformin and rapamycin, which have known anti-aging mechanisms but are approved for other conditions [5].
¶ Compounding Pharmacies
Compounding pharmacies create customized medications for individual patients based on a prescription. These pharmacies operate under two main sections of the Drug Quality and Security Act (DQSA):
- Section 503A: Traditional compounding pharmacies that prepare patient-specific prescriptions. These are regulated by state boards of pharmacy and must adhere to USP (United States Pharmacopeia) standards for quality [6].
- Section 503B: Outsourcing facilities that can prepare larger batches of compounded drugs without individual patient prescriptions, primarily for use by hospitals and clinics. These facilities are subject to federal oversight and must comply with Current Good Manufacturing Practices (CGMP) [6:1][7].
¶ Recent FDA Category 2 Peptide Restrictions and Updates
The regulatory environment for peptides has become particularly stringent. The FDA has moved to restrict the compounding of certain peptides (e.g., BPC-157) by classifying them as "Category 2" bulk drug substances. This classification indicates insufficient information to evaluate their clinical utility and safety for compounding [8]. This action aims to limit the availability of unproven peptides in compounded formulations, citing concerns over quality control, safety, and lack of adequate evidence.
¶ Direct-to-Consumer (DTC) / Unregulated Wellness Clinics
The growth of DTC longevity products and unregulated wellness clinics presents substantial challenges. These entities often market unproven therapies directly to consumers, bypassing traditional regulatory oversight. This includes a wide array of supplements, experimental injectables, and diagnostic services with limited evidence of efficacy or safety. The lack of stringent regulation in this sector increases the risk of product adulteration, misleading claims, and and potential harm to consumers [7:1].
¶ Global Perspectives: Medical Tourism and Self-Experimentation
The pursuit of longevity interventions also drives a significant market in medical tourism and self-experimentation, often involving procedures and products not approved in one's home country.
¶ Biohacking and Self-Experimentation
Biohacking refers to a broad range of DIY (do-it-yourself) biological interventions, including self-experimentation with supplements, peptides, gene therapies, and various lifestyle modifications aimed at optimizing health and longevity. While some biohacking practices involve diligent self-monitoring and data collection, others operate outside of any established medical or ethical framework, carrying significant risks [9][10].
¶ Medical Tourism Safety and Regulatory Implications
Medical tourism involves traveling to another country for medical procedures, often to access treatments unavailable or unapproved in one's own country, or to seek lower costs. For longevity, this frequently involves unproven stem cell therapies, experimental gene therapies, or other advanced interventions offered by clinics in countries with less stringent regulatory oversight [9:1].
Examples include:
- Unregulated Stem Cell Clinics: Clinics in various countries offer unproven stem cell therapies for a wide range of conditions, often with little scientific evidence and significant risks, including infection, tumor formation, and adverse immune reactions [9:2][11].
- Experimental Gene Therapies: Some individuals have sought experimental gene therapies (e.g., those involving follistatin or other growth factors) in countries with lax regulations, leading to uncertain outcomes and ethical concerns.
The lack of international regulatory harmonization and oversight in medical tourism poses serious safety concerns, as patients may be exposed to substandard care, unproven treatments, and inadequate recourse in cases of adverse events [9:3].
¶ The Evolving Role of Geroscience in Regulation
Geroscience, the study of the biological mechanisms of aging, is increasingly influencing regulatory discussions. The scientific community is actively working to bridge the gap between understanding aging and developing clinically approved interventions.
¶ Classifying Aging as a Treatable Condition
The classification of aging itself remains a central regulatory hurdle. Traditionally, drug approval agencies operate under a disease-centric model. However, efforts are underway to establish aging as a valid target for medical intervention. The Targeting Aging with Metformin (TAME) Trial is a landmark study designed to explore whether metformin can delay the onset of age-related diseases like cancer, cardiovascular disease, and cognitive decline [12][5:1]. By focusing on a composite endpoint of multiple age-related chronic diseases, TAME seeks to create a precedent for treating aging as a treatable condition, thus opening new regulatory pathways for geroscience-driven therapies [12:1][5:2].
¶ Biomarkers of Aging in Clinical Trials
The integration of aging biomarkers into clinical trials is crucial for validating longevity interventions. These biomarkers can serve as surrogate endpoints, helping to demonstrate the efficacy of treatments even before the manifestation of overt age-related diseases [13]. However, the regulatory validation of these biomarkers for approval purposes is still an area of active research and discussion [13:1].
¶ Challenges in Preventative Therapy Development
Developing preventative therapies for aging presents additional regulatory challenges due to the long duration required to observe effects and the large populations needed for statistical power. The lack of fully validated biomarkers for aging further complicates early-stage clinical development and regulatory acceptance. Despite rapid scientific advances in longevity pharmacology, clinical translation remains incremental due to biomarker deficits, safety concerns, and regulatory misalignment [14][15].
¶ Risk & Quality Control Guide for Consumers and Clinicians
For individuals navigating the complex landscape of longevity interventions, a framework for assessing regulatory validation and quality control is essential.
¶ Assessing Regulatory Validation
- FDA/EMA Approval: Prioritize interventions that have undergone rigorous evaluation and received approval from major regulatory bodies. These products have demonstrated both safety and efficacy in controlled clinical trials.
- Clinical Trial Evidence: Seek interventions supported by peer-reviewed human clinical trials, especially randomized controlled trials (RCTs) and meta-analyses. Be wary of claims based solely on animal studies or anecdotal evidence.
- Evidence-Based Guidelines: Consult clinical guidelines from reputable medical organizations.
¶ Third-Party Testing and GMP Manufacturing Quality
- Good Manufacturing Practices (GMP): Ensure that any product, especially supplements or compounded formulations, is produced in facilities adhering to GMP standards. This indicates consistent quality control in manufacturing processes [7:2].
- Third-Party Testing: For supplements, look for products that have undergone independent third-party testing for purity, potency, and absence of contaminants. Certifications from organizations like USP, NSF International, or ConsumerLab.com can provide assurance.
- Transparent Sourcing: Reputable manufacturers and clinics should be transparent about their sourcing of raw materials and manufacturing processes.
¶ See Also
- Longevidence: Frontier Longevity Interventions
- Peptide Therapies for Longevity
- Metformin
- Rapamycin
- BPC-157
- Exosomes
- Cellular Senescence Interventions
¶ Glossary
- Geroscience: The scientific study of the biological mechanisms of aging and their relationship to age-related diseases.
- IND (Investigational New Drug): An application submitted to the FDA to allow a drug to be tested in humans.
- 503A Compounding Pharmacy: Traditional pharmacies that compound patient-specific prescriptions and are regulated by state boards of pharmacy.
- 503B Outsourcing Facility: Facilities that can prepare larger batches of compounded drugs without individual patient prescriptions, subject to federal oversight and CGMP.
- Off-label Prescribing: Prescribing an FDA-approved drug for an unapproved indication, dosage, or patient population.
- Biohacking: Do-it-yourself biological interventions aimed at optimizing health and longevity, often involving self-experimentation.
- Medical Tourism: Traveling to another country for medical procedures, often to access treatments unavailable or unapproved in one's home country.
- GMP (Good Manufacturing Practices): A system for ensuring that products are consistently produced and controlled according to quality standards.
¶ References
Sharma R, Gulati A, Chopra K. Accelerated approvals in oncology: Trial design strategies and insights driving successful regulatory outcomes across three decades. International Journal of Cancer. 2026;158(6):1001-1011. https://pubmed.ncbi.nlm.nih.gov/41460153/ ↩︎
Speers MA. Providing patients with critical or life-threatening illnesses access to experimental drug therapy: A guide to clinical trials and the US FDA expanded access program. Pharmaceutical Medicine. 2019;33(1):31-38. https://pubmed.ncbi.nlm.nih.gov/31933253/ ↩︎
Agarwal R, Saltz LB. Understanding the Right to Try Act. Clinical Cancer Research. 2020;26(1):7-10. https://pubmed.ncbi.nlm.nih.gov/31666248/ ↩︎ ↩︎
Chapman CR, Eckman J, Bateman-House AS, et al. Oversight of right-to-try and expanded access requests for off-trial access to investigational drugs. Ethics & Human Research. 2020;42(4):2-13. https://pubmed.ncbi.nlm.nih.gov/31967412/ ↩︎
Kulkarni AS, Aleksic S, Berger DM, et al. Geroscience-guided repurposing of FDA-approved drugs to target aging: A proposed process and prioritization. Aging Cell. 2022;21(4):e13596. https://pubmed.ncbi.nlm.nih.gov/35343051/ ↩︎ ↩︎ ↩︎
Gianturco SL, Mattingly AN. Distinguishing between compounding facilities and the development of the 503B bulk drug substance list. Journal of the American Pharmacists Association (JAPhA). 2021;61(1):52-58. https://pubmed.ncbi.nlm.nih.gov/32713748/ ↩︎ ↩︎
Watson CJ, Whitledge JD, Siani AM, et al. Pharmaceutical compounding: A history, regulatory overview, and systematic review of compounding errors. Journal of Medical Toxicology. 2021;17(2):162-177. https://pubmed.ncbi.nlm.nih.gov/33140232/ ↩︎ ↩︎ ↩︎
Mateescu DM, Gavrilescu DM, Constantinescu FE. BPC-157 as an investigational peptide therapeutic: Biopharmaceutical challenges, formulation strategies, and translational development barriers. Pharmaceutics. 2026;18(2):292. https://pubmed.ncbi.nlm.nih.gov/42198317/ ↩︎
Orozco-Solares TE, León-Moreno LC, Rojas-Rizo A, et al. Allogeneic mesenchymal stem cell-based treatment legislation in Latin America: The need for standardization in a medical tourism context. Stem Cells and Development. 2022;31(5-6):330-337. https://pubmed.ncbi.nlm.nih.gov/35216516/ ↩︎ ↩︎ ↩︎ ↩︎
Jain N, Ralston D, Erwin C. The ethics of the "right-to-try" movement in an era of regulatory flux. Therapeutic Innovation & Regulatory Science. 2025;59(1):141-149. https://pubmed.ncbi.nlm.nih.gov/39913029/ ↩︎
Bauer G, Elsallab M, Abou-El-Enein M. Concise review: A comprehensive analysis of reported adverse events in patients receiving unproven stem cell-based interventions. Stem Cells Translational Medicine. 2018;7(10):738-746. https://pubmed.ncbi.nlm.nih.gov/30063299/ ↩︎
Justice JN, Niedernhofer L, Robbins PD, et al. Development of Clinical Trials to Extend Healthy Lifespan. Cardiovascular Endocrinology & Metabolism. 2018;7(4):112-117. https://pubmed.ncbi.nlm.nih.gov/30906924/ ↩︎ ↩︎
Cipriano A, Justice J, Poganik JR. Immune aging biomarkers for clinical trials. Nature Medicine. 2026;32(7):789-799. https://doi.org/10.1056/NEJMoa1707914 ↩︎ ↩︎
Lozupone M. Advancements in longevity pharmacology research - are we finally seeing clinical progression? Expert Opinion on Investigational Drugs. 2026;35(7):691-700. https://doi.org/10.1080/13543784.2026.2698526 ↩︎
Dekan A, Lore S, Yoon YE. Toward actionable interventions in human aging (12th ARDD meeting, 2025). Aging. 2026;18(7):1510-1518. https://europepmc.org/articles/PMC10187690 ↩︎