¶ Lasers, IPL, and Energy Devices
Lasers, Intense Pulsed Light (IPL), and other Energy-Based Devices (EBDs) form the core of modern aesthetic and interventional dermatology. By delivering targeted electromagnetic, thermal, or sound energy into the skin, these modalities stimulate tissue remodeling, coagulate aberrant blood vessels, and destroy unwanted pigment or follicular targets.
This guide outlines the classification, biophysical mechanisms, and clinical outcomes of therapeutic light and energy devices, mapping technology classes to skin indications, safety profiles (including the Fitzpatrick scale), and post-procedure protocols.
| Mechanism | Selective Photothermolysis, Controlled Thermal Remodeling |
| Key Spec | Wavelength (nm), Pulse Duration, Fluence, Target Chromophore |
| Protocol | Series of 3–6 sessions, spaced 2–6 weeks apart |
| FDA Class | Class II / Class IV (clinical devices) |
| Entry Cost | $150–$1,500+ per session (in-clinic) |
¶ TL;DR
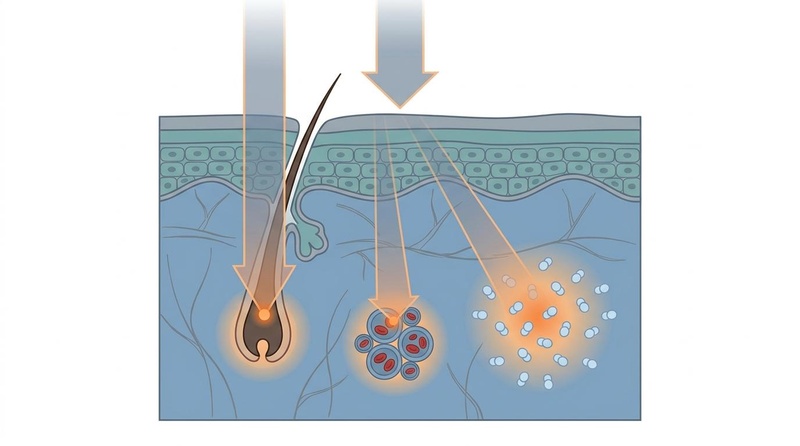
- Selective Target Selection: EBDs rely on selective photothermolysis, matching specific wavelengths to target chromophores—melanin (pigment/hair), hemoglobin (redness/vessels), or water (collagen/resurfacing) [1].
- Aesthetic Phenotype Mapping: Device selection is strictly governed by the patient's presenting phenotype and Fitzpatrick skin type, with vascular devices treating erythema and ablative or non-ablative fractional devices targeting textural damage [2].
- Combination Synergy: Simultaneously combining neuromodulators like Botulinumtoxin A with fractional laser resurfacing significantly enhances wrinkle reduction by minimizing post-treatment mechanical tension during collagen deposition [1:1].
- Risk Profile: Fitzpatrick skin types IV–VI (skin of color) face elevated risks of post-inflammatory hyperpigmentation (PIH) and scarring, necessitating specialized wavelengths (e.g., Nd:YAG 1064 nm) and conservative param choices [3].
- Clinical Evidence Limitations: High-certainty systematic review and network meta-analysis evidence supports vascular EBDs for rosacea, while combinations or rare dermatological conditions have highly localized, emerging data bases [2:1], [4]. RF microneedling and microfocused ultrasound offer effective alternatives for skin tightening and scar remodeling, especially in darker skin types [5], [3:1], [6].
¶ Quick Answer
Energy-Based Devices (EBDs) treat a wide array of skin conditions through targeted, energy-mediated tissue alteration. Vascular systems such as Pulsed Dye Lasers (PDL, 595 nm) and Intense Pulsed Light (IPL, 500–1200 nm) target hemoglobin to coagulate and clear facial erythema and telangiectasias [2:2]. Pigment systems and hair removal lasers target melanin to resolve solar lentigines or arrest follicular development [1:2]. Resurfacing devices (fractional CO2, Erbium:YAG) use water as a chromophore, vaporizing or heating skin columns to induce neo-collagenesis for scar and wrinkle remodeling [4:1]. Radiofrequency microneedling (RFMN) and microfocused ultrasound (MFU) offer non-light based alternatives, delivering energy directly to the dermis or SMAS layer, making them suitable for all Fitzpatrick skin types, including IV–VI [6:1], [3:2]. Fitzpatrick skin types I–III are optimal candidates for most light-based wavelengths, whereas types IV–VI require long-pulsed Nd:YAG (1064 nm) or non-light modalities (radiofrequency, ultrasound) to bypass epidermal melanin and prevent thermal injury [3:3].
¶ Identify the Type: Candidate Fit and Modality Mapping
The clinical utility of energy-based modalities is governed by the biophysical interaction between the device's energy profile and the patient's individual cutaneous characteristics. Selecting the appropriate device requires matching the specific skin concern to the optimal chromophore target, while factoring in safety limits defined by the Fitzpatrick scale, expected downtime, and protective parameters.
¶ Modality Selection Matrix
| Modality Class | Primary Skin Concerns | Target Chromophore / Tissue Layer | Fitzpatrick Skin Type Safety | Downtime Profile | Adverse-Event Prevention Strategy |
|---|---|---|---|---|---|
| Intense Pulsed Light (IPL) | Superficial redness, mild pigment, photoaging, and long-term hair removal. | Melanin (follicle/epidermis), Hemoglobin. | Safe: Types I–III. High Risk: Types IV–VI (epidermal burns). |
Minimal (0–24 hours of mild erythema). | Use cutoff filters to exclude shorter wavelengths; cooling templates. |
| Vascular Lasers (e.g., PDL 595nm, KTP 532nm) | Persistent redness, rosacea, and broken capillaries [2:3], morphea [4:2]. | Oxyhemoglobin in dermal capillaries. | Safe: Types I–III. Caution: Types IV–V (longer pulse width required). |
Mild swelling, potential purpura/bruising (3–7 days). | Dynamic cooling devices (DCD); long pulse durations to limit purpuric damage. |
| Pigment Lasers (e.g., Q-Switched, Picosecond) | Lentigines, tattoos, blemishes, pigment marks, and acne scars, post-inflammatory hyperpigmentation. | Melanin (melanosomes / dermal ink). | Safe: Types I–III. Moderate Risk: Types IV–VI (requires low fluences). |
Minimal (mild crusting for 2–5 days). | Select picosecond pulse widths over nanosecond to reduce thermal diffusion. |
| Fractional Ablative Lasers (e.g., CO2, Er:YAG) | Deep wrinkles, atrophic scars, severe texture, morphea [4:3]. | Water (epidermal vaporization & deep dermal heating). | Safe: Types I–III. High Risk: Types IV–VI (severe PIH, keloid scarring). |
Significant (5–10 days of oozing, peeling, erythema). | Prophylactic antivirals; topical tyrosinase inhibitors; low density settings. |
| Fractional Non-Ablative (e.g., Er:Glass 1540/1550nm) | Mild wrinkles, early scars, morphea [4:4], or general dull skin, enlarged pores, and uneven texture [7], [5:1]. | Water (creates coagulation columns, spares stratum corneum). | Moderate Safety: Types I–V. Caution: Type VI (requires lower energy). |
Moderate (1–3 days of swelling and redness). | Cryogen cooling; conservative density and energy settings. |
| Radiofrequency Microneedling (RFMN) | Skin laxity, acne scars, deeper wrinkles and skin elasticity, texture [8], [9]. | Dermal water / structural collagen (bypasses epidermal melanin). | Highly Safe: Types I–VI (excellent option for skin of color) [3:4]. | Mild (2–4 days of erythema and dry texture). | Insulated needles to protect the epidermis from thermal conduction. |
| Microfocused Ultrasound (MFU / Ultherapy) | Skin laxity, submental lifting, jawline definition [6:2], [10], [11]. | SMAS (Superficial Muscular Aponeurotic System) / Deep Dermis. | Highly Safe: Types I–VI (no melanin interaction). | Negligible (mild deep muscle soreness for 1–2 weeks). | Precise visualization of facial layers to avoid skeletal muscle or bone heating. |
¶ Evidence Snapshot
¶ Evidence Summary Table (Human Outcomes)
The clinical evidence supporting EBDs in clinical dermatology varies across indications. While systematic reviews of randomized controlled trials (RCTs) support vascular lasers and IPL for rosacea, evidence for rare autoimmune conditions or novel combinations relies on smaller trials or systematic reviews of observational cohorts.
| Clinical Outcome | Device / Intervention | Observed Effect | Consistency of Data | Certainty of Evidence (GRADE) | Key Findings & Caveats | Primary Citations |
|---|---|---|---|---|---|---|
| Erythema & Telangiectasia Reduction (Rosacea) | Vascular Lasers (PDL, KTP) & IPL | Significant clearance of superficial erythema and dilated capillaries. | High | High | PDL is highly effective for telangiectasias; combining devices with topical medications is recommended for patients presenting with multiple rosacea phenotypes [2:4]. | [2:5] |
| Reduction of Morphea Plaque Thickness | Pulsed Dye Laser (PDL), Fractional Lasers (CO2, Er:YAG), Excimer | Moderate reduction in plaque induration and improvement in skin elasticity. | Moderate | Low | Evidence limited to systematic reviews of case series and small cohorts. PDL (8 studies) and fractional lasers (6 studies) show favorable safety, but lack massive RCT verification [4:5]. | [4:6] |
| Facial & Periorbital Wrinkle Remodeling | Combined Botulinum Toxin A (BTX-A) & Laser Resurfacing (CO2/Er:YAG) | Significantly superior clinical improvement compared to laser monotherapy. | Moderate | Moderate | BTX-A pretreatment (1–6 weeks prior) paralyzes underlying musculature, reducing movement during skin healing. Small RCTs (10–33 patients) support adjunctive benefit [1:3]. | [1:4] |
| Skin Tightening & Laxity (Face/Neck) | Microfocused Ultrasound (MFU) | Significant non-invasive lifting and tightening of the lower face and neck, with sustained results. | High | Moderate | MFU creates thermal coagulation points at precise depths (e.g., SMAS) to induce collagen denaturation and neocollagenesis [6:3], [10:1], [11:1]. | [6:4], [10:2], [11:2] |
| Acne Scar & Skin Texture Remodeling | Radiofrequency Microneedling (RFMN) | Significant improvement in atrophic acne scars, skin texture, and pore size, with minimal downtime. | High | Moderate | RFMN induces controlled thermal injury in the dermis, stimulating collagen and elastin production. Effective for all skin types [8:1], [9:1], [3:5]. | [8:2], [9:2], [3:6] |
| Neck Rejuvenation (Wrinkles & Laxity) | RF Microneedling vs. Fractional Non-Ablative Laser | Comparable efficacy in reducing neck wrinkles and improving skin laxity, with RFMN having better safety for darker skin. | Moderate | Moderate | Both modalities stimulate neocollagenesis. RFMN often preferred for shorter recovery and reduced PIH risk in Fitzpatrick IV-VI [5:2], [7:1]. | [5:3], [7:2] |
| Carbon Footprint Mitigation in Practice | Energy-Based Devices (EBDs) | Reductions in clinical waste, disposable tips, and idle standby energy draw. | Moderate | Moderate | Environmental audits show EBDs represent a measurable share of dermatological carbon footprints; procedural efficiency and recycling decrease impacts [12]. | [12:1] |
¶ What Causes It or How It Works: Biophysical Principles
To understand how energy-based devices interact with biological tissues, clinicians and operators must master three core concepts: the target chromophores, selective photothermolysis, and non-light-based physical remodeling.
¶ Target Chromophores and Absorption Wavelengths
A chromophore is an endogenous light-absorbing molecule in the skin. The three primary chromophores targeted in aesthetic medicine are:
- Melanin: Located in the epidermis and hair follicles. It has a broad absorption spectrum, peaking in the ultraviolet range and steadily declining through the visible and near-infrared (NIR) spectra (250–1200 nm).
- Hemoglobin: Found within erythrocytes in dermal blood vessels. It exhibits strong absorption peaks in the blue (418 nm), green (542 nm and 577 nm), and near-infrared ranges.
- Water: The main constituent of dermal tissue. Its absorption is negligible in visible light but increases dramatically in the mid-infrared to far-infrared ranges (above 1300 nm, with massive peaks at 1940 nm, 2940 nm, and 10,600 nm).
¶ The Principle of Selective Photothermolysis
Established by Anderson and Parrish, this principle dictates that selective thermal destruction of a target structure is achieved when:
- Wavelength Selectivity: The light wavelength penetrates deeply enough and is absorbed preferentially by the target chromophore rather than surrounding structures.
- Thermal Relaxation Time (TRT): The energy is delivered in a pulse duration shorter than or equal to the TRT of the target structure. The TRT is the time required for the target to lose 50% of its heat to surrounding tissue. Keeping pulse duration under the TRT prevents collateral thermal damage (burns/scarring).
- Sufficient Fluence: The energy density (fluence, measured in ) is high enough to damage the target structure but within the safety thresholds of the surrounding epidermis.
¶ Non-Light Energy Mechanics (Radiofrequency & Ultrasound)
Unlike lasers and IPL, radiofrequency and ultrasound do not rely on light absorption or chromophores.
- Radiofrequency (RF): Employs alternating electrical currents that flow through the tissue. Because the tissue resists this electrical current (impedance), heat is generated according to Ohm's Law. This thermal energy is concentrated in the deep dermis, causing immediate collagen helix contraction and triggering a sub-acute wound-healing response that promotes neocollagenesis [3:7].
- Microfocused Ultrasound (MFU): Utilizes acoustic waves focused precisely onto deep dermal or fascial layers (the SMAS). The ultrasound waves cause rapid friction among molecules, generating localized, intense heat (60–70°C) at micro-thermal zones, leading to tissue contraction and tight fascial lifting [6:5].
¶ Starter Protocol: Parameter Setup & Post-Care
Because parameter settings vary dramatically by device manufacturer, the following parameters are representative clinical guidelines for typical aesthetic indications.
¶ 1. Pre-Treatment Preparation (4 Weeks Prior)
- Melanin Suppression: For Fitzpatrick skin types IV–VI, initiate topical tyrosinase inhibitors (e.g., azelaic acid, cysteamine, or low-dose hydroquinone) to downregulate melanocyte activity and prevent post-inflammatory hyperpigmentation (PIH) and rebound melasma; see post-inflammatory hyperpigmentation and melasma for detailed clinical preparation.
- UV Avoidance: Complete sun avoidance. Active tanning activates epidermal melanocytes, dramatically increasing the risk of superficial blistering or depigmentation.
- Discontinue Retinoids: Pause topicals like tretinoin or glycolic acid 5–7 days before energy-based procedures to stabilize the stratum corneum.
¶ 2. General Standard Procedural Parameters (Representative)
Vascular Laser (PDL 595 nm) --- Wavelength: 595 nm
--- Fluence: 6.0–8.5 J/cm²
--- Pulse Duration: 6.0–20.0 ms
--- Cooling: DCD 30 ms spray / 20 ms delay
Pigment Laser (QS Nd:YAG) --- Wavelength: 1064 nm (deep) / 532 nm (epidermal)
--- Spot Size: 3.0–5.0 mm
--- Pulse Duration: nanosecond or picosecond
--- Fluence: 1.5–3.5 J/cm²
Fractional CO2 (Ablative) --- Wavelength: 10,600 nm
--- Energy: 15–40 mJ per beam
--- Treatment Density: 5%–15% coverage
--- Pulse Mode: Ultra-pulsed / Fractional
¶ 3. Immediate Post-Procedure Protocol (Days 1–7)
- Barrier Restoration: Apply physiological lipid-barrier ointments (containing ceramides, cholesterol, and free fatty acids) or medical-grade petrolatum multiple times daily to prevent trans-epidermal water loss (TEWL) and assist in preventing and minimizing scars.
- Gentle Cleansing: Wash twice daily with a non-foaming, lipid-free, syndet cleanser. Avoid physical friction or washcloths.
- Photoprotection: After the skin barrier has re-epithelialized (usually day 2 for non-ablative, day 5–7 for ablative), enforce strict application of broad-spectrum, mineral-only (zinc oxide/titanium dioxide) sunscreens.
¶ Stronger Add-On Path: Advanced Combination Protocols
Clinical efficacy is substantially boosted by combining energy-based procedures with neuromodulators, autologous growth factors, or specialized topical formulations.
¶ Neuromodulator (BTX-A) & Resurfacing Combinations
Injecting Botulinumtoxin A (BTX-A) 1 to 6 weeks prior to, or simultaneously with, facial laser resurfacing significantly improves the remodeling of dynamic and static wrinkles [1:5].
- Biological Mechanism: Laser resurfacing vaporizes dermal layers and initiates intense collagen remodeling over several months. Repetitive facial expressions during this healing phase create mechanical tension across the newly forming collagen strands, causing them to heal in a folded or wrinkled pattern.
- Clinical Outcomes: By temporarily paralyzing local muscle fibers, BTX-A minimizes mechanical movement. The newly synthesized collagen fibers are deposited in an unwrinkled, organized, and parallel orientation [1:6]. Prospective clinical trials demonstrate a statistically superior cosmetic improvement on the side pretreated with BTX-A compared to the laser-only side [1:7].
¶ Energy-Based Delivery of Topicals (LADD)
Laser-Assisted Drug Delivery (LADD) utilizes fractional ablative lasers (usually Er:YAG or low-fluence CO2) to create microscopic ablation channels. Immediately following channel creation, active topicals (such as sterile formulations of vitamin C, tranexamic acid, or growth factors) are applied. These channels bypass the lipophilic stratum corneum, allowing large molecules to penetrate directly into the deep dermis, amplifying therapeutic responses for pigmentation or scarring.
¶ Clinical/Procedure Path
Medical-grade energy-based devices (Class IIIb and Class IV lasers) are strictly regulated and must be administered within a clinical setting by licensed, trained professionals.
- Initial Clinical Clearance: Patients presenting with autoimmune skin diseases such as lupus erythematosus, dermatomyositis, or localized scleroderma (morphea) require careful clinical triage [4:7], [13]. Although some studies show lasers can safely improve morphea plaques, active systemic inflammation or skin lesions driven by lupus carry risks of photo-induced flares, requiring close coordinate care [4:8], [13:1].
- Parameter Customization: Clinical assessment of skin thickness, vascularity, and melanin density determines the exact energy level, spot size, and cooling duration. Standardized treatment protocols are modified based on real-time tissue response (e.g., immediate transient erythema, mild purpura, or tissue graying).
¶ What Usually Fails: Common Roadblocks & Non-Responders
Energy-based treatments are not universally successful. Identifying the reasons for suboptimal outcomes is critical for managing non-responders:
- Over-treating Melasma with Aggressive Light Wavelengths: Melasma is highly sensitive to heat. Applying aggressive, high-fluence lasers or standard IPL often triggers intense melanocyte rebound, worsening hyperpigmentation. Gentle, low-fluence picosecond lasers or topical tyrosinase inhibitors are preferred.
- Using Light Devices on Dark Skin (Fitzpatrick IV–VI): Attempting to remove hair or treat scars using standard Alexandrite (755 nm) or IPL devices in skin of color often results in severe epidermal burns, blistering, and subsequent permanent hypopigmentation or severe PIH [3:8].
- Incomplete Treatment Cycles: Conditions like deep scars or skin laxity require multiple sessions (typically 3–6) spaced 4–6 weeks apart. Patients who discontinue treatment after 1 or 2 sessions often report treatment failure because collagen remodeling takes 3 to 6 months to mature.
- Inadequate Cooling and Operator Speed Errors: Moving a laser handpiece too slowly or failing to calibrate cooling sprays (DCD) leads to heat accumulation in the epidermis, converting a safe, localized dermal treatment into a deep, scarring thermal burn.
¶ Tracking Plan
To maintain objectivity and document therapeutic outcomes, clinicians and patients should implement a structured tracking framework:
- Standardized Clinical Photography: Take high-resolution images in identical lighting, using consistent facial angles (frontal, 45-degree, and 90-degree profiles) and matching camera settings before every session and 3 months post-completion.
- Wood's Lamp / Cross-Polarized Imaging: Utilize cross-polarized photography to isolate deep vascular patterns, or a Wood's Lamp (365 nm) to assess the depth of hyperpigmentation (distinguishing epidermal pigment, which enhances, from dermal pigment, which does not).
- Downtime Log: Record the duration (in hours or days) of post-procedure erythema, swelling, purpura, and peeling to assist in setting parameters for subsequent sessions.
- Patient-Reported Outcome Measures (PROMs): Utilize validated aesthetic scales to grade patient satisfaction, subjective skin texture improvements, and pain scores.
¶ Safety and Red Flags
The clinical operation of Class IV lasers and EBDs demands strict adherence to rigorous safety standards:
¶ Ocular Safety
- Wavelength-Specific Protective Eyewear: Both the patient and all clinical staff within the nominal hazard zone must wear goggles certified for the specific laser wavelength being fired. Standard safety glasses or closing the eyes does not prevent permanent retinal or corneal blindness.
- Corneal Shields: For procedures performed within the orbital rim (e.g., periorbital resurfacing), intraocular stainless steel corneal shields must be inserted under topical ophthalmic anesthesia.
¶ Absolute Contraindications
- Active Cutaneous Infection: Treating over active herpes simplex virus, impetigo, or open, unepithelialized wounds is contraindicated.
- Isotretinoin Therapy: Patients must wait 6 months after completing oral isotretinoin before undergoing aggressive ablative laser resurfacing to avoid atypical scarring.
- Photosensitizing Medications: Active use of tetracyclines, amiodarone, or other systemic photosensitizers requires postponing light-based procedures.
- Keloidal Tendency: History of keloid formation represents a relative to absolute contraindication for deep ablative resurfacing.
¶ Clinical Red Flags and Complications
In professional practice, certain clinical indicators signify severe complications requiring immediate clinical intervention or adjustment of treatment protocols:
- Atypical Blistering: Signifies epidermal-dermal separation from excessive thermal energy or poor epidermal cooling.
- Sustained Erythema & Purpura: Erythema persisting beyond 72 hours for non-ablative or 14 days for ablative treatments, or unexpected deep purpura.
- Secondary Infection: Indicated by pustules, crusting, localized exquisite tenderness, or constitutional signs. Post-operative herpes simplex reactivation requires prophylactic antiviral therapies.
- Severe Dyspigmentation: Broad hyperpigmentation (PIH) or permanent hypopigmentation (depigmentation).
¶ FAQs
¶ What is the difference between laser and IPL?
A laser emits a single, highly focused, coherent wavelength of light, making it highly specific for a single target (e.g., 595 nm for red blood vessels) [1:8]. IPL emits a broad spectrum of non-coherent light (usually 500–1200 nm) filtered to target multiple concerns (pigment and redness) simultaneously but with less specificity [1:9].
¶ Why is Fitzpatrick skin typing so important?
The Fitzpatrick scale measures skin melanin density and response to UV light. Lighter skin types (I–III) have less epidermal melanin and can tolerate aggressive light treatments safely. Darker skin types (IV–VI) have abundant epidermal melanin, which acts as a competing chromophore, absorbing light intended for deeper targets and causing burns, blistering, and PIH if incorrect devices are used [3:9].
¶ Can radiofrequency microneedling be performed on dark skin?
Yes. Unlike lasers, radiofrequency energy does not target melanin. The electrical energy is delivered via insulated needles directly into the dermis, bypassing the pigment-rich epidermis, making RF microneedling exceptionally safe for Fitzpatrick skin types IV–VI [3:10].
¶ How many laser treatments are typically required?
While superficial pigment spots or small blood vessels may resolve in 1 or 2 sessions, complex concerns like acne scarring, deep wrinkles, rosacea erythema, and hair removal typically require 3 to 6 sessions to achieve significant clinical clearance [2:6]. For conditions like skin laxity and deeper scars treated with RF microneedling or microfocused ultrasound, multiple sessions (e.g., 3-6) are also typically needed for optimal collagen remodeling and sustained results [6:6].
¶ Is there any way to reduce the environmental footprint of these procedures?
Yes. Professional clinics can reduce their carbon footprint by utilizing energy-efficient standby modes on EBD platforms, optimizing the use of reusable cooling guides where sterile protocols permit, and implementing clinic-wide recycling of non-hazardous procedural packaging [12:2].
¶ References
Chan K, Singh P, Dhar S, Mutsago T, Elahi T, Mosahebi A. Botulinum A Toxin and Laser Therapy: Evidence and Recommendations for Combination Treatment. Aesthetic Surgery Journal. 2023 Sep;43(10):NP811-NP814. https://pubmed.ncbi.nlm.nih.gov/37427871/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Nguyen L, Sorbe C, Seeber N. Laser and energy-based devices for treating rosacea - a systematic review and network meta-analysis. Journal der Deutschen Dermatologischen Gesellschaft (JDDG). 2026 Jan. https://pubmed.ncbi.nlm.nih.gov/41273013/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Syder NC, Chen A, Elbuluk N. Radiofrequency and Radiofrequency Microneedling in Skin of Color: A Review of Usage, Safety, and Efficacy. Dermatologic Surgery. 2023 May 1;49(5):540-545. https://pubmed.ncbi.nlm.nih.gov/36826381/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Szczepanik-Kułak P, Michalska-Jakubus M, Krasowska D. Laser Therapy for the Treatment of Morphea: A Systematic Review of Literature. Journal of Clinical Medicine. 2021 Jul;10(15):3409. https://pubmed.ncbi.nlm.nih.gov/34362192/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Almukhtar R, Wood E, Goldman M, Fabi SG, Boen M. The Efficacy and Safety of Radiofrequency Microneedling Versus a Nonablative Fractional 1,550-nm Erbium:Glass Laser for the Rejuvenation of the Neck. Dermatologic Surgery. 2022 Sep 1;48(9):980-984. https://pubmed.ncbi.nlm.nih.gov/36054046/ ↩︎ ↩︎ ↩︎ ↩︎
Wang R, Peng G, Chen Y, Shao X, Liu L, Chen T, Shi M, Zhong J, Ou Y, Chen J. Combined Novel Microfocused Ultrasound and Microneedle Fractional Radiofrequency System for Multilayered Facial Rejuvenation: A Prospective, Randomized, and Split-Face Study. Journal of Cosmetic Dermatology. 2025 Oct. https://pubmed.ncbi.nlm.nih.gov/40980871/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Dou W, Yang Q, Yin Y. Fractional microneedle radiofrequency device and fractional erbium-doped glass 1,565-nm device treatment of human facial photoaging: a prospective, split-face, random clinical trial. Journal of Cosmetic and Laser Therapy. 2021 Aug;23(5):291-297. https://pubmed.ncbi.nlm.nih.gov/35083965/ ↩︎ ↩︎ ↩︎
Kumar N, Suh DH, Lee SJ. Radiofrequency Microneedling for Facial Rejuvenation: A Systematic Review. Journal of Cosmetic Dermatology. 2026 Apr. https://pubmed.ncbi.nlm.nih.gov/41947517/ ↩︎ ↩︎ ↩︎
Niaz G, Ajeebi Y, Alshamrani HM. Fractional Radiofrequency Microneedling as a Monotherapy in Acne Scar Management: A Systematic Review of Current Evidence. Clinical, Cosmetic and Investigational Dermatology. 2025. https://pubmed.ncbi.nlm.nih.gov/39781098/ ↩︎ ↩︎ ↩︎
Wood E, Gonzalez A, Almukhtar R, Fabi SG. Comparing the Safety and Effectiveness of Microfocused Ultrasound: Standard vs Targeted Tissue Protocol in Lifting and Tightening the Lower Face and Upper Neck. Journal of Drugs in Dermatology (JDD). 2024 Apr 1;23(4):S4-S10. https://pubmed.ncbi.nlm.nih.gov/38564386/ ↩︎ ↩︎ ↩︎
Alhaddad M, Wu DC, Bolton J. A Randomized, Split-Face, Evaluator-Blind Clinical Trial Comparing Monopolar Radiofrequency Versus Microfocused Ultrasound With Visualization for Lifting and Tightening of the Face and Upper Neck. Dermatologic Surgery. 2019 Jan;45(1):127-134. https://pubmed.ncbi.nlm.nih.gov/30531187/ ↩︎ ↩︎ ↩︎
Karakoyun Ö, Ayhan E, Aydın D. Carbon footprint assessment of Energy-Based devices in clinical and aesthetic dermatology. Lasers in Medical Science. 2025 Sep. https://pubmed.ncbi.nlm.nih.gov/40973842/ ↩︎ ↩︎ ↩︎
Joh HC, Jue MS, Ko JY. Energy-Based Devices for the Treatment of Cutaneous Lesions in Patients With Lupus Erythematosus and Dermatomyositis. Journal of Cosmetic Dermatology. 2026 Jan. https://pubmed.ncbi.nlm.nih.gov/41521846/ ↩︎ ↩︎