¶ Reversing Hair Loss
Reversing hair loss is possible when the follicle is still alive. The hard part is matching the treatment to the cause: androgenetic alopecia, telogen effluvium, traction, inflammation, autoimmune alopecia, nutritional deficiency, medication effect, postpartum shedding, thyroid disease, iron deficiency, or scarring disease. Pattern hair loss usually needs a long-term growth signal plus a long-term anti-miniaturization signal. Diffuse shedding usually needs the trigger removed. Scarring alopecia needs urgent medical control before the follicle is permanently replaced by scar tissue.
¶ TL;DR
- Best-supported core stack for male pattern hair loss: topical or oral minoxidil plus a 5-alpha-reductase inhibitor such as finasteride or dutasteride, with photos, labs when appropriate, and 12 months of consistency before judging.[1][2][3]
- Best-supported core stack for female pattern hair loss: topical minoxidil is first-line; low-dose oral minoxidil, spironolactone, finasteride, or dutasteride may be considered off-label with clinician oversight, pregnancy prevention, and cause-specific workup.[4][5][6]
- Best add-ons: Platelet-Rich Plasma (PRP), red light therapy, and microneedling, with ketoconazole shampoo when dandruff/inflammation is present, and hair transplantation for stable donor supply and advanced pattern loss.[7][8][9][10]
- Supplements help mainly when you are deficient. Systematic nutrition assessment, correcting deficiencies in iron, vitamin D, and zinc, and optimizing biotin (if deficient) matter; random "hair vitamins" rarely fix androgen-driven miniaturization.[11][12]
- Tissue Remodeling & Growth Support: Peptides like GHK-Cu show promise in preclinical models for follicle enlargement and microvascular support, often explored as premium cosmetic adjuncts.[13]
- Scarring, patchy, painful, rapidly progressive, or inflamed hair loss is not a cosmetic project. It needs dermatology evaluation quickly, because delay can cost follicles permanently.[14]
- Holistic Aesthetic Context: Hair health is a major pillar of the broader Appearance Hub, which coordinates skin, scar, and scalp optimization protocols.
¶ Quick Answer
Fastest Useful First Steps for Men with Pattern Hair Loss
- Document: Take clear, consistent photos (front, top, temples) every 1-3 months to track progress.
- Minoxidil: Start 5% topical minoxidil once daily.
- DHT Control: Discuss oral finasteride 1mg/day or topical finasteride with a clinician if male pattern loss is aggressive.
- Targeted Supplements: Only if deficient – check iron, vitamin D, zinc. Avoid random "hair vitamins." See Nutrition.
- Scalp Health: Treat any dandruff or irritation with ketoconazole shampoo.
- Patience: Commit for at least 6-12 months before evaluating efficacy.
Fastest Useful First Steps for Women with Pattern Hair Loss
- Document: Take clear, consistent photos (part, front, temples) every 1-3 months.
- Minoxidil: Start 5% topical minoxidil once daily.
- Evaluate underlying causes: Discuss potential issues like iron deficiency, thyroid problems, PCOS, and perimenopause with a clinician.
- Targeted Supplements: Only if deficient – check ferritin, vitamin D, zinc. See Nutrition.
- Scalp Health: Treat any dandruff or irritation with ketoconazole shampoo.
- Patience: Commit for at least 6-12 months before evaluating efficacy.
For common pattern hair loss, the most evidence-based plan is: confirm the diagnosis, photograph the scalp, start minoxidil, add androgen control when appropriate, treat scalp inflammation, correct deficiencies, and reassess at 6 and 12 months. PRP, red light therapy, and microneedling can improve response, but they work best as add-ons rather than substitutes for proven pharmacology. Hair transplant surgery can restore density where follicles are gone, but it does not stop future miniaturization; maintenance therapy still matters.
¶ First: Identify the Type of Hair Loss
Hair is a cycling organ. Follicles rotate through anagen (growth), catagen (regression), and telogen (resting/shedding). Hair loss happens when follicles miniaturize, shed too many hairs at once, become inflamed, are pulled out mechanically, or are destroyed by scarring disease.
| Pattern | What it looks like | Common causes | First move |
|---|---|---|---|
| Temple/crown thinning in men | Receding hairline, crown spot, preserved sides/back | Androgenetic alopecia | Minoxidil plus DHT suppression discussion |
| Widening part in women | Central part widening, ponytail smaller, hairline often preserved | Female pattern hair loss, low ferritin, thyroid, PCOS, menopause | Workup plus minoxidil; consider antiandrogen |
| Sudden diffuse shedding | Handfuls in shower, starts 2-4 months after trigger | Telogen effluvium, illness, crash diet, postpartum, medication | Find and remove trigger; correct deficiency |
| Round patches | Smooth circular bald patches | Alopecia areata | Dermatology; steroids/JAK inhibitor discussion |
| Pain, burning, scale, pustules, shiny scalp | Hair loss plus inflammation or loss of follicle openings | Scarring alopecia, infection, lupus, lichen planopilaris | Urgent dermatology |
| Edges/hairline traction | Thinning where hairstyles pull | Braids, extensions, tight buns, helmets | Stop traction early |
¶ Evidence Snapshot
| Therapy | Best use | Effect | Confidence | Notes |
|---|---|---|---|---|
| Topical minoxidil | Men and women with pattern hair loss | High | FDA-approved; improves hair count and density, but requires ongoing use.[1:1][4:1] | |
| Oral low-dose minoxidil | Pattern hair loss when topical is irritating or impractical | Moderate | Off-label; growing evidence, but monitor edema, tachycardia, hypertrichosis, blood pressure.[5:1] | |
| Finasteride | Male pattern hair loss; selected postmenopausal women off-label | High in men, lower in women | Reduces DHT and slows miniaturization; pregnancy contraindication for women who could become pregnant.[2:1][6:1] | |
| Dutasteride | Stronger DHT suppression, usually off-label for hair | Moderate | Often more potent than finasteride but longer half-life and similar antiandrogen precautions.[3:1] | |
| Spironolactone | Female pattern hair loss with androgen features | Low to Moderate | Useful in women with acne, hirsutism, PCOS features, or hyperandrogenism; avoid in pregnancy.[6:2] | |
| PRP | Add-on for androgenetic alopecia | Moderate | Meta-analyses show density/count gains, but protocols vary substantially.[7:1] | |
| Red light therapy | Add-on or medication-sparing support | Moderate | FDA-cleared devices exist; results require months and consistent use.[8:1][15] | |
| Microneedling | Add-on to minoxidil or PRP | Moderate | Can improve outcomes, likely through wound-healing signals and delivery enhancement.[9:1] | |
| Ketoconazole shampoo | Dandruff/seborrheic dermatitis plus pattern loss | Low | Best as scalp-inflammation support, not a standalone regrowth therapy.[10:1] | |
| Hair transplantation | Advanced stable pattern loss with good donor area | High for cosmetic density | Moves resistant follicles; does not prevent native hair from continuing to miniaturize.[16] | |
| Supplements & Nutrition | Deficiency-related shedding | High for deficiency, low without deficiency | Correct iron, vitamin D, zinc, protein, thyroid, and diet issues; avoid blind biotin or multi megadosing.[11:1][12:1] | |
| Exosomes, stem-cell media, SVF | Experimental regenerative approaches | Low | Interesting early studies, but regulation, product quality, dosing, and long-term safety remain unresolved.[17] | |
| Scalp massage | Low-risk support | Very Low | Small studies suggest possible thickness changes; not a replacement for proven therapy.[18] |
¶ The Core Biology
Pattern hair loss is not just "hair falling out." In androgenetic alopecia, genetically susceptible follicles respond to dihydrotestosterone (DHT) and local signaling changes by shrinking over repeated cycles. A thick terminal hair becomes a finer, shorter, less pigmented hair. Eventually the follicle can become cosmetically invisible.
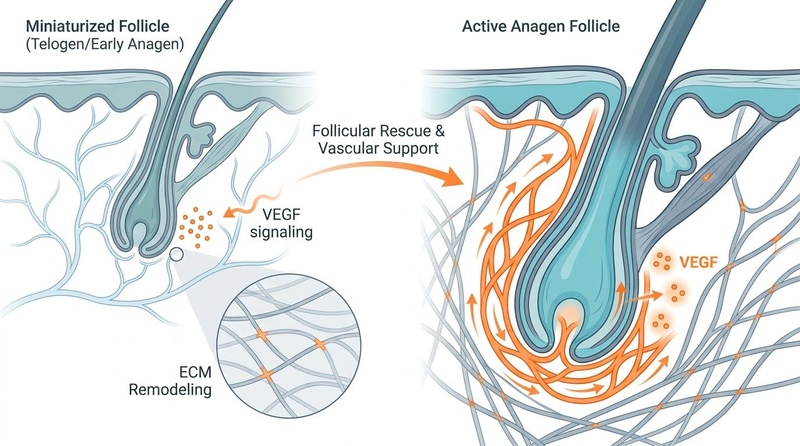
Within the follicular microenvironment, reversing hair loss relies on shifting follicles from a miniaturized state back into a prolonged, active anagen phase. This transformation requires coordinated signals across several pathways:
- Microvascular Support & VEGF Signaling: Miniaturized follicles exhibit decreased capillary density. Upregulating vascular endothelial growth factor (VEGF) is critical to stimulate angiogenesis, supplying oxygen and nutrients to the active hair bulb. Growth supports like Platelet-Rich Plasma (PRP) and red light therapy enhance local blood flow and mitochondrial respiration, encouraging vascular remodeling.[7:2][8:2]
- Extracellular Matrix (ECM) Remodeling: For a follicle to physically expand during the transition to active growth, the surrounding dermal sheath and extracellular matrix must be remodeled. Signaling molecules such as copper tripeptides like GHK-Cu support this tissue remodeling and help enlarge hair follicles in preclinical models.[13:1]
- Systemic Metabolic Integrity: Follicles cannot sustain rapid cellular division without adequate cofactors. Optimizing core micronutrients like biotin (if deficient), zinc, iron, and vitamin D ensures cellular energy and protein synthesis pathways are unimpeded.[11:2][12:2]
The main reversible levers are:
- Keep follicles in anagen longer: minoxidil, red light therapy, PRP, microneedling, and possibly melatonin act partly through growth-phase support.[1:2][8:3][9:2][19]
- Reduce androgen pressure: finasteride and dutasteride lower DHT; spironolactone blocks androgen signaling in women.[2:2][3:2][6:3]
- Improve scalp environment: treat seborrheic dermatitis, psoriasis, folliculitis, traction, inflammation, and irritant reactions.[10:2][14:1]
- Correct systemic bottlenecks: nutrition baseline optimization (for iron, vitamin D, zinc, protein, thyroid status, and biotin if deficient) addresses key metabolic drivers of shedding.[11:3][12:3]
- Replace lost density: transplantation moves follicles from resistant donor areas to cosmetically important regions.[16:1]
¶ Men: Practical Evidence-Based Protocol
¶ Starter Protocol
- Document baseline: front hairline, temples, crown, mid-scalp, and wet-hair photos under the same light every month.
- Use minoxidil consistently: 5% foam or solution once daily is often easier to sustain than twice daily. Early shedding can happen in the first 2-8 weeks.
- Discuss DHT control: finasteride 1 mg/day is the classic oral regimen; some clinicians use lower oral doses or topical finasteride to reduce systemic exposure.[2:3][20]
- Treat scalp inflammation: dandruff, itching, redness, scale, or seborrheic dermatitis can sabotage adherence and hair appearance. Ketoconazole 1-2% shampoo 2-3 times weekly is commonly used.[10:3]
- Judge at 12 months: many people see shedding reduction by 3-4 months, visible density by 6-12 months, and maximum cosmetic effect after 12-18 months.
¶ Stronger Add-On Path
- Platelet-Rich Plasma (PRP): often 3-4 monthly sessions, then maintenance every 3-6 months. Ask about platelet concentration, leukocyte content, spin system, activation method, and photo-tracking.[7:3]
- Microneedling: commonly 0.5-1.5 mm weekly or every 1-2 weeks in studies and clinics, adjusted for tolerance. Do not apply irritating topicals immediately after deeper needling unless supervised.[9:3]
- Red Light Therapy: use an LLLT helmet/cap/comb with published parameters or FDA clearance, usually 3-4 sessions weekly for at least 16-26 weeks.[8:4]
- Dutasteride: discuss if finasteride response is inadequate or aggressive loss continues. It suppresses type I and II 5-alpha-reductase more strongly, but is off-label in many settings and persists longer in the body.[3:3]
¶ Women: Practical Evidence-Based Protocol
Female hair loss needs more diagnostic care because diffuse shedding, low ferritin, thyroid disease, PCOS, perimenopause, postpartum changes, autoimmune disease, and medication effects can mimic or worsen female pattern hair loss.
¶ Starter Protocol
- Confirm pattern: central part widening, Christmas-tree pattern, bitemporal recession, diffuse thinning, or shedding dominant?
- Check common contributors: Baseline nutrition screen (CBC, ferritin/iron studies, TSH, vitamin D, zinc, and biotin when indicated), menstrual history, postpartum timing, diet, medications, acne/hirsutism/irregular cycles, and signs of inflammation.[11:4][12:4]
- Start topical minoxidil: 5% foam once daily is widely used for women; irritation and unwanted facial hair are the common adherence problems.[4:2]
- Consider oral options with a clinician: low-dose oral minoxidil, spironolactone, finasteride, or dutasteride can be considered in selected women, especially postmenopausal women or women using reliable contraception.[5:2][6:4]
- Do not use antiandrogens during pregnancy attempts, pregnancy, or breastfeeding unless a specialist explicitly says so. Finasteride and dutasteride are contraindicated because of fetal risk.
¶ When Women Benefit Most From Antiandrogen Strategy
Antiandrogens are most plausible when hair loss coexists with acne, oily skin, hirsutism, PCOS, high androgens, perimenopausal acceleration, or strong family pattern hair loss. Spironolactone is commonly used off-label; finasteride/dutasteride are more restricted because of pregnancy risk and mixed evidence in premenopausal women.[6:5]
¶ Therapies, Ranked by Role
¶ Minoxidil
Minoxidil is a growth-phase support drug. It opens potassium channels, supports dermal papilla signaling, and can increase hair shaft diameter and count. It does not remove the androgen driver, which is why men with aggressive pattern hair loss often need DHT control too.[1:3]
Topical advantages: FDA-approved, inexpensive, local effect, good long-term safety.
Topical downsides: daily mess, scalp irritation, propylene glycol sensitivity, shedding phase, unwanted facial hair if it runs onto the face.
Oral low-dose advantages: easier adherence and useful when topical fails from irritation.
Oral low-dose downsides: off-label; can cause hypertrichosis, ankle swelling, fast heartbeat, dizziness, fluid retention, and blood pressure changes.[5:3]
¶ Finasteride and Dutasteride
Finasteride inhibits type II 5-alpha-reductase, lowering scalp and serum DHT. Dutasteride inhibits type I and II and is usually more potent, but with longer persistence. These are the most direct tools for androgen-driven follicle miniaturization.[2:4][3:4]
Key cautions: sexual side effects, mood concerns, breast tenderness, semen parameter changes in some men, PSA interpretation changes, and pregnancy contraindication for women who could become pregnant. A clinician should interpret risks and alternatives.
¶ Topical Finasteride
Topical finasteride aims to reduce scalp DHT with less systemic exposure. Evidence supports biologic activity and clinical benefit, but formulations vary and it is still not as standardized as oral finasteride.[20:1]
¶ Spironolactone
Spironolactone blocks androgen receptors and lowers androgen effects. It is mostly used for women, especially when acne, PCOS features, or androgen excess are present. Monitor for dizziness, menstrual changes, breast tenderness, potassium issues in higher-risk patients, and pregnancy risk.[6:6]
¶ Platelet-Rich Plasma (PRP)
PRP concentrates platelets from your own blood and injects growth-factor-rich plasma into the scalp. It may support dermal papilla cells, angiogenesis, and anagen signaling. The evidence is promising, but "PRP" is not one thing: platelet dose, leukocyte content, spin system, activation, injection depth, and maintenance schedule vary.[7:4] See the full Platelet-Rich Plasma (PRP) Guide for a detailed breakdown.
Best fit: people with early-to-moderate androgenetic alopecia who want an add-on and can afford repeated sessions.
Weak fit: complete bald areas, scarring alopecia without disease control, or anyone expecting a one-session cure.
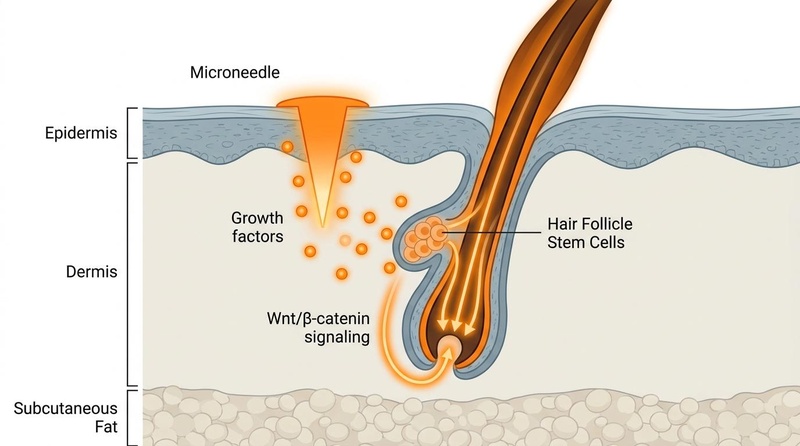
¶ Microneedling
Microneedling creates controlled micro-injury. In the scalp, this may activate wound-healing pathways, Wnt/beta-catenin signaling, platelet/growth factor activity, and topical delivery. Trials often combine microneedling with minoxidil and show better outcomes than minoxidil alone.[9:4] Check out our comprehensive Microneedling Guide for depths, frequencies, and hygiene protocols.
Safety rules: avoid active infection, psoriasis flares, severe seborrheic dermatitis, keloid tendency, anticoagulation concerns, or unsupervised deep needling. Clean technique matters.
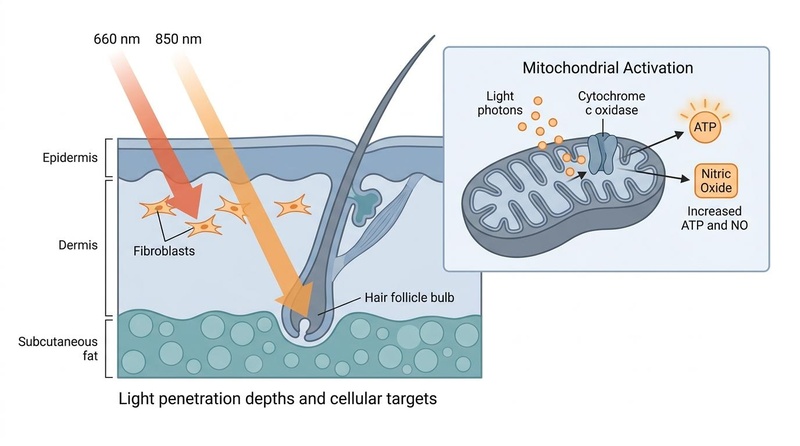
¶ Red Light Therapy and Low-Level Laser Therapy
Photobiomodulation uses red or near-infrared light to influence mitochondrial signaling, inflammation, and hair cycling. The strongest hair-loss evidence is for androgenetic alopecia with consistent device use for months.[8:5] Read the Red Light Therapy Guide for more details on specific wavelengths and parameters.
Practical point: the device you actually use for 6 months beats the perfect device left in a drawer.
¶ Ketoconazole and Scalp Inflammation Control
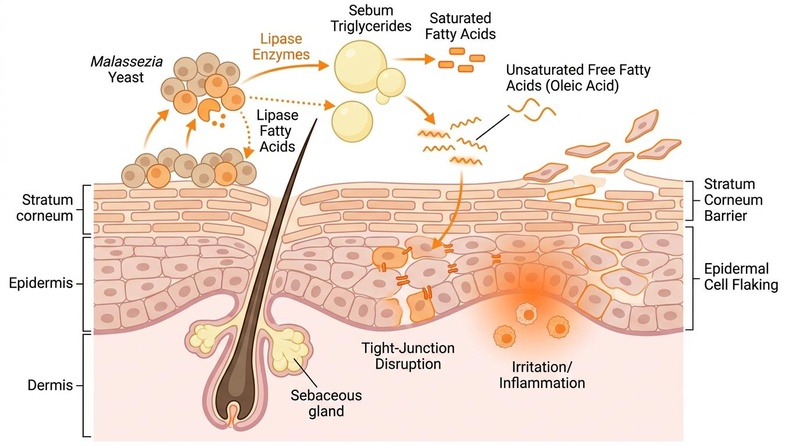
Ketoconazole shampoo can reduce Malassezia-driven dandruff and scalp inflammation. It may have mild antiandrogen or anti-inflammatory effects, but the best reason to use it is a calmer scalp that tolerates other therapies.[10:4]
¶ Hair Transplantation
Follicular unit extraction (FUE) and follicular unit transplantation (FUT) move androgen-resistant follicles from donor zones to thin areas. This can be transformative, but it is redistribution, not regeneration. The donor supply is finite. Future native hair loss can make a transplant look unnatural unless medical therapy stabilizes the pattern.[16:2]
¶ Supplements and Nutrient Correction
Supplements are powerful when they correct a real bottleneck and mostly disappointing when they are used as magic dust. See the Nutrition Guide for systematic dietary structuring.
| Candidate | When it matters | What to check | Caution |
|---|---|---|---|
| Iron | Heavy periods, vegetarian/vegan diet, postpartum, fatigue, diffuse shedding | CBC, ferritin, iron studies | Iron overload is harmful; supplement based on labs.[11:5] |
| Vitamin D | Low sun exposure, darker skin at high latitude, autoimmune risk, deficiency | 25(OH)D | Correct deficiency; do not megadose blindly.[12:5] |
| Zinc | Deficiency, malabsorption, restrictive diet | Zinc, diet history | Excess zinc can cause copper deficiency.[12:6] |
| Protein/energy | Crash dieting, GLP-1 appetite suppression, eating disorder risk, endurance dieting | Diet history, weight change | Telogen effluvium often follows rapid weight loss. |
| Biotin | True deficiency is rare | Deficiency risk, brittle nails, diet | High-dose biotin can distort lab tests, including thyroid and cardiac tests.[12:7] |
| Omega-3, antioxidants, saw palmetto | Adjunctive or experimental | Product quality, drug interactions | Evidence is much weaker than minoxidil or antiandrogens. |
¶ GHK-Cu and Copper Peptides
GHK-Cu has plausible follicle biology: dermal papilla support, VEGF signaling, and in vitro effects on hair-related cells. The human evidence is not yet strong enough to rank it with minoxidil, finasteride, PRP, or transplant. It belongs in the "promising but not foundational" category.[13:2] Read our full GHK-Cu Profile for tissue-remodeling science and topical formulations.
¶ Topical Melatonin
Topical melatonin has small clinical studies suggesting reduced shedding and possible improvement in androgenetic alopecia or diffuse alopecia. It is low-cost and biologically plausible, but evidence remains limited compared with the core therapies.[19:1]
¶ Heat, Cold, Massage, and Circulation Tools
Scalp massage may modestly increase hair thickness in small studies, possibly through mechanical stimulation of dermal papilla cells. Heat and cold exposure have no strong direct evidence for reversing androgenetic alopecia. They may support general health, stress physiology, or scalp comfort, but should not displace proven treatment.[18:1]
¶ Peptides, Exosomes, Stem Cells, and Conditioned Media
This is the frontier zone. Exosomes, adipose-derived stromal vascular fraction, stem-cell conditioned media, and peptide signals are scientifically interesting because hair follicles are regenerative mini-organs. The problem is not plausibility; it is standardization, regulation, dose, purity, durability, and long-term safety. Treat these as experimental unless done in a legitimate clinical/research setting.[17:1]
¶ Sex and Age Differences
Hair loss clinical presentations and safety windows vary dramatically across age groups and biological sex:
¶ Young Adults (Ages 18–35)
- Men: Early-onset androgenetic alopecia (AGA) in young men is often highly aggressive due to elevated levels of 5-alpha-reductase activity. Early stabilization with oral 5-alpha-reductase inhibitors (finasteride) is highly prioritized to rescue follicles before irreversible miniaturization and fibrosis occur.[2:5]
- Women: Diffuse thinning in young women is frequently linked to nutritional deficiencies (especially iron deficiency/ferritin below 40 ng/mL) or hormonal fluctuations related to oral contraceptives, Polycystic Ovary Syndrome (PCOS), or postpartum telogen effluvium.[4:3][11:6] Pregnancy safety is a non-negotiable threshold: antiandrogens (finasteride, spironolactone) must be strictly avoided due to risks of teratogenicity.
¶ Middle-Aged Adults (Ages 36–60)
- Men: Receding temples and crown thinning progress but often at a steadier rate. Combination therapies (minoxidil + finasteride + microneedling) yield the highest response rates.[9:5][20:2]
- Women: Menopause acts as a major biological trigger for female pattern hair loss (FPHL). As estrogen levels decline, the relative protective effect of estrogens against circulating androgens is diminished. Postmenopausal women may use spironolactone or off-label finasteride with reduced systemic concern, under medical supervision.[6:7]
¶ Older Adults (Ages 60+)
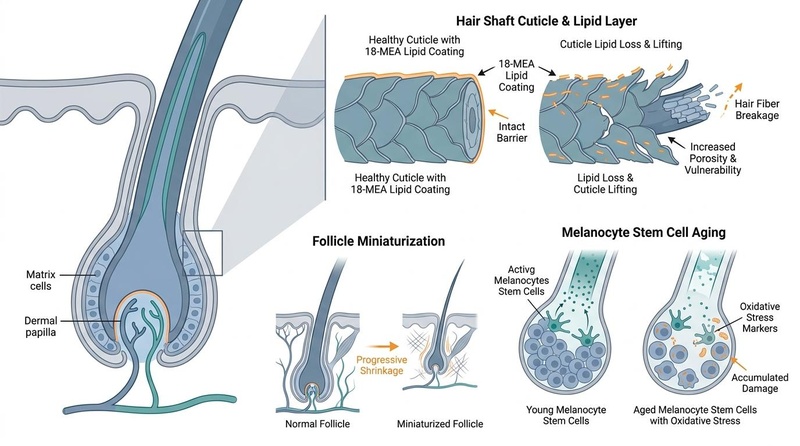
- Both Sexes: "Senescent alopecia" represents age-related hair thinning that occurs independent of genetic androgen sensitivity. It is characterized by progressive lipid loss in the hair shaft, follicle miniaturization, and exhaustion of hair follicle stem cells.[17:2] Growth signaling aids like low-level light therapy (PBM) and GHK-Cu, which stimulate capillary networks without systemic drug-interaction risks, are highly favored as primary or supportive treatments.[8:6][13:3]
¶ What Usually Fails
- Starting five interventions at once, then not knowing what worked.
- Quitting minoxidil during the early shed.
- Using PRP or red light therapy as a substitute for DHT control in aggressive male pattern hair loss.
- Buying supplements without checking ferritin, thyroid, vitamin D, diet, or medication triggers.
- Waiting years with scarring symptoms: pain, burning, pustules, smooth shiny scalp, or loss of follicle openings.
- Getting a transplant before stabilizing ongoing loss.
- Applying irritating topicals to an already inflamed scalp.
¶ Decision Tree
¶ Tracking Plan
| Metric | How | Frequency | Why |
|---|---|---|---|
| Standard photos | Same room, light, hair length, wet/dry status | Monthly | Prevents mood-based judgment |
| Shed count | Shower/brush estimate, not obsessive counting | Weekly | Detects trend, not daily noise |
| Scalp symptoms | Itch, burn, scale, oil, tenderness | Weekly | Inflammation changes adherence and diagnosis |
| Hair shaft diameter/density | Dermoscopy or clinic phototrichogram | Every 3-6 months | Best objective progress marker |
| Labs when indicated | CBC, ferritin, TSH, vitamin D, zinc, androgens | Baseline and follow-up | Finds correctable bottlenecks |
¶ Safety and Red Flags
Talk to a clinician before using prescription therapies, combining procedures, or treating hair loss during pregnancy planning, pregnancy, or breastfeeding.
Urgent evaluation is warranted for:
- Sudden patchy loss.
- Pain, burning, pus, crust, bleeding, or significant scale.
- Eyebrow, eyelash, beard, or body-hair loss with scalp changes.
- Smooth shiny skin where follicle openings are disappearing.
- Hair loss with severe fatigue, weight change, menstrual disruption, virilization, anemia symptoms, or thyroid symptoms.
- New hair loss after starting medication, major illness, surgery, GLP-1 weight loss, crash dieting, or chemotherapy.
¶ FAQs
¶ Can hair loss really be reversed?
Yes, if follicles are miniaturized or dormant rather than destroyed. Pattern hair loss can often be slowed and partially reversed. Scarring alopecia destroys follicles, so early disease control matters more than later regrowth promises.
¶ How long before I know if treatment works?
Use 6 months for early signal and 12 months for a fair judgment. Hair grows slowly, and early shedding can look worse before it looks better.
¶ Is minoxidil forever?
For androgenetic alopecia, usually yes. Minoxidil-supported hairs are often lost after stopping because the underlying biology remains.
¶ Is finasteride required for men?
Not always, but it is the most direct evidence-based way to reduce DHT-driven miniaturization. Men with aggressive temple/crown loss usually need to at least consider it.
¶ What is different for women?
Women need more attention to diffuse shedding triggers, iron status, thyroid disease, postpartum timing, PCOS features, perimenopause, and pregnancy safety. Topical minoxidil is still foundational.
¶ Does PRP beat minoxidil?
PRP can help, but it is usually best as an add-on. It is more expensive and less standardized than minoxidil.
¶ Does red light therapy work?
It can modestly improve density in androgenetic alopecia when used consistently for months. It is not a fast fix, and device quality matters. Read the Red Light Therapy Guide for more details.
¶ Should I microneedle at home?
Shallow cosmetic needling is lower risk, but deeper scalp needling can cause infection, irritation, scarring, or worsen inflammation if done poorly. If using it with minoxidil or PRP, get a clinician-guided protocol. Check out our comprehensive Microneedling Guide for depths, frequencies, and hygiene protocols.
¶ Methods
This guide prioritizes human clinical trials, systematic reviews, meta-analyses, dermatology reviews, and safety guidance available through PubMed, PubMed Central, major dermatology journals, and established clinical references. Evidence strength is graded higher when effects are replicated in controlled human studies and lower when based on small uncontrolled studies, animal work, in vitro mechanisms, or heterogeneous procedure protocols.
¶ References
¶ Update Log
- 2026-07-03: Created full evidence-based guide and added generated biomedical follicle pathway image.
- 2026-07-04: Updated cross-links, added distinct 'Fastest Useful First Steps' callout boxes for men and women, integrated detailed scientific pathways of follicular transition, and replaced the top image with a new generated Nano Banana Pro illustration for follicular rescue, microvascularization (VEGF), and ECM remodeling.
- 2026-07-07: Performed image audit and enrichment. Integrated multiple professional diagrams (hair quality mechanisms, microneedling hair growth pathway, red-light-therapy penetration depth, scalp Malassezia pathophysiology) to match section contexts. Expanded clinical details on sex and age differences across the lifespan.
Suchonwanit P, Thammarucha S, Leerunyakul K. Minoxidil and its use in hair disorders: a review. Drug Design, Development and Therapy. 2019. https://pmc.ncbi.nlm.nih.gov/articles/PMC6691938/ ↩︎ ↩︎ ↩︎ ↩︎
Adil A, Godwin M. The effectiveness of treatments for androgenetic alopecia: a systematic review and meta-analysis. Journal of the American Academy of Dermatology. 2017. https://pubmed.ncbi.nlm.nih.gov/28396101/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Zhou Z, Song S, Gao Z, Wu J, Ma J, Cui Y. The efficacy and safety of dutasteride compared with finasteride in treating men with androgenetic alopecia: a systematic review and meta-analysis. Clinical Interventions in Aging. 2019. https://pmc.ncbi.nlm.nih.gov/articles/PMC6388756/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
van Zuuren EJ, Fedorowicz Z, Schoones J. Interventions for female pattern hair loss. Cochrane Database of Systematic Reviews. 2016. https://pubmed.ncbi.nlm.nih.gov/27225981/ ↩︎ ↩︎ ↩︎ ↩︎
Randolph M, Tosti A. Oral minoxidil treatment for hair loss: a review of efficacy and safety. Journal of the American Academy of Dermatology. 2021. https://pubmed.ncbi.nlm.nih.gov/32622136/ ↩︎ ↩︎ ↩︎ ↩︎
Carmina E, Azziz R, Bergfeld W, et al. Female pattern hair loss and androgen excess: a report from the Multidisciplinary Androgen Excess and PCOS Committee. Journal of Clinical Endocrinology & Metabolism. 2019. https://pubmed.ncbi.nlm.nih.gov/30785988/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Gupta AK, Bamimore MA, Foley KA. Efficacy of platelet-rich plasma in androgenetic alopecia: systematic review and meta-analysis. Journal of Dermatological Treatment. 2022. https://pubmed.ncbi.nlm.nih.gov/34854395/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Afifi L, Maranda EL, Zarei M, et al. Low-level laser therapy as a treatment for androgenetic alopecia. Lasers in Surgery and Medicine. 2017. https://pubmed.ncbi.nlm.nih.gov/28335213/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Fertig RM, Gamret AC, Cervantes J, Tosti A. Microneedling for the treatment of hair loss? Journal of the European Academy of Dermatology and Venereology. 2018. https://pubmed.ncbi.nlm.nih.gov/29194786/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Piérard-Franchimont C, De Doncker P, Cauwenbergh G, Piérard GE. Ketoconazole shampoo: effect of long-term use in androgenic alopecia. Dermatology. 1998. https://pubmed.ncbi.nlm.nih.gov/9669136/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Trost LB, Bergfeld WF, Calogeras E. The diagnosis and treatment of iron deficiency and its potential relationship to hair loss. Journal of the American Academy of Dermatology. 2006. https://pubmed.ncbi.nlm.nih.gov/16635664/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Almohanna HM, Ahmed AA, Tsatalis JP, Tosti A. The role of vitamins and minerals in hair loss: a review. Dermatology and Therapy. 2019. https://pmc.ncbi.nlm.nih.gov/articles/PMC6380979/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Pyo HK, Yoo HG, Won CH, et al. The effect of tripeptide-copper complex on human hair growth in vitro. Archives of Pharmacal Research. 2007. https://pubmed.ncbi.nlm.nih.gov/17687679/ ↩︎ ↩︎ ↩︎ ↩︎
Mirmirani P, Tosti A, Goldberg L, Whiting D, Sotoodian B. Primary cicatricial alopecia: diagnosis and treatment. Canadian Family Physician. 2011. https://pmc.ncbi.nlm.nih.gov/articles/PMC3247865/ ↩︎ ↩︎
Tantiyavarong J, Charoensuksira S, Meephansan J, et al. Red and Green LED Light Therapy: A Comparative Study in Androgenetic Alopecia. Photodermatology, Photoimmunology & Photomedicine. 2024. https://pubmed.ncbi.nlm.nih.gov/39368074/ ↩︎
Jimenez F, Alam M, Vogel JE, Avram M. Hair transplantation: basic overview. Journal of the American Academy of Dermatology. 2021. https://pubmed.ncbi.nlm.nih.gov/33259833/ ↩︎ ↩︎ ↩︎
Gupta AK, Renaud HJ, Quinlan EM, Shear NH, Piguet V. The use of platelet-rich plasma, stem cells, and exosomes in the treatment of androgenetic alopecia. Journal of Cosmetic Dermatology. 2020. https://pubmed.ncbi.nlm.nih.gov/32510754/ ↩︎ ↩︎ ↩︎
Koyama T, Kobayashi K, Hama T, Murakami K, Ogawa R. Standardized scalp massage results in increased hair thickness by inducing stretching forces to dermal papilla cells. Eplasty. 2016. https://pmc.ncbi.nlm.nih.gov/articles/PMC4740347/ ↩︎ ↩︎
Fischer TW, Trüeb RM, Hänggi G, Innocenti M, Elsner P. Topical melatonin for treatment of androgenetic alopecia. International Journal of Trichology. 2012. https://pmc.ncbi.nlm.nih.gov/articles/PMC3681103/ ↩︎ ↩︎
Piraccini BM, Blume-Peytavi U, Scarci F, et al. Topical finasteride spray solution for male androgenetic alopecia: a phase III randomized controlled trial. Journal of the European Academy of Dermatology and Venereology. 2022. https://pubmed.ncbi.nlm.nih.gov/34634163/ ↩︎ ↩︎ ↩︎